

Relative carcinogenicity of tacrolimus vs mycophenolate after solid organ transplantation and its implications for liver transplant care
- PMID: 38689747
- PMCID: PMC11056899
- DOI: 10.4254/wjh.v16.i4.650
Relative carcinogenicity of tacrolimus vs mycophenolate after solid organ transplantation and its implications for liver transplant care
Abstract
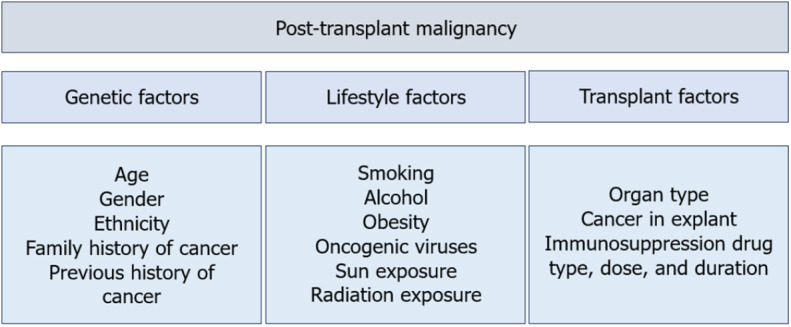
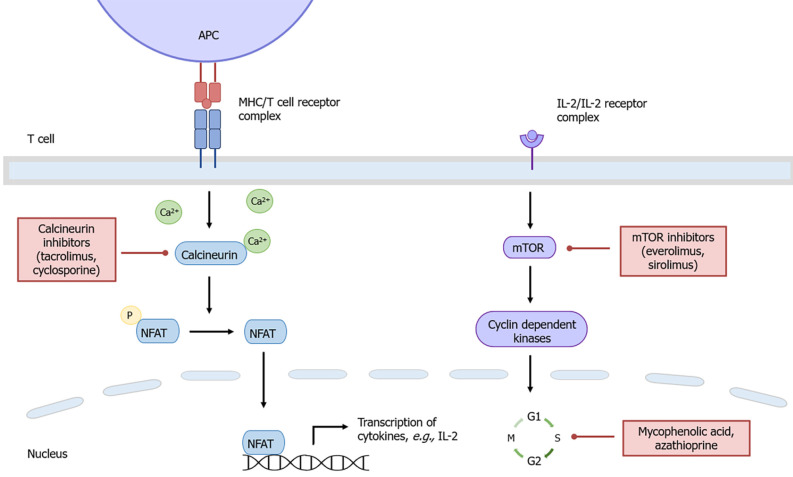
Background: De novo malignancy is a leading cause of late morbidity and mortality in liver transplant recipients. Cumulative immunosuppression has been shown to contribute to post-transplant malignancy (PTM) risk. There is emerging evidence on the differential carcinogenic risk profile of individual immunosuppressive drugs, independent of the net effect of immunosuppression. Calcineurin inhibitors such as tacrolimus may promote tumourigenesis, whereas mycophenolic acid (MPA), the active metabolite of mycophenolate mofetil, may limit tumour progression. Liver transplantation (LT) is relatively unique among solid organ transplantation in that immunosuppression monotherapy with either tacrolimus or MPA is often achievable, which makes careful consideration of the risk-benefit profile of these immunosuppression agents particularly relevant for this cohort. However, there is limited clinical data on this subject in both LT and other solid organ transplant recipients.
Aim: To investigate the relative carcinogenicity of tacrolimus and MPA in solid organ transplantation.
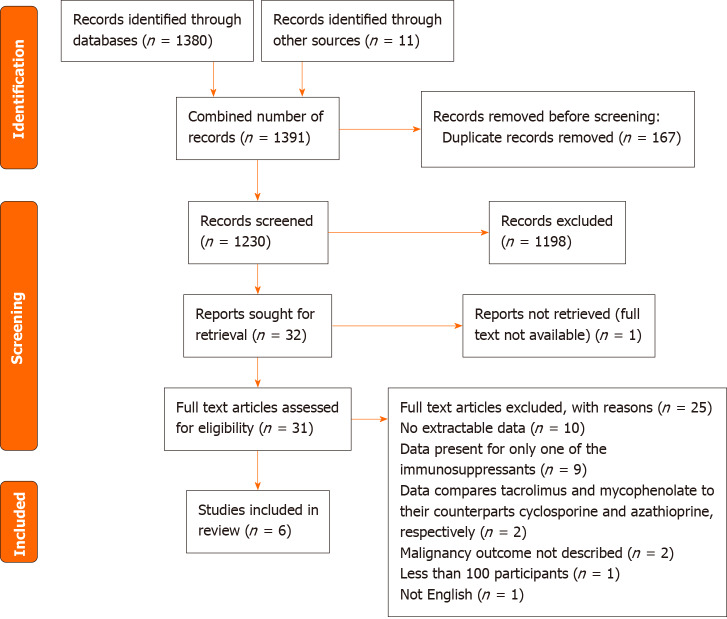
Methods: A literature search was conducted using MEDLINE and Embase databases using the key terms "solid organ transplantation", "tacrolimus", "mycophenolic acid", and "carcinogenicity", in order to identify relevant articles published in English between 1st January 2002 to 11th August 2022. Related terms, synonyms and explosion of MeSH terms, Boolean operators and truncations were also utilised in the search. Reference lists of retrieved articles were also reviewed to identify any additional articles. Excluding duplicates, abstracts from 1230 records were screened by a single reviewer, whereby 31 records were reviewed in detail. Full-text articles were assessed for eligibility based on pre-specified inclusion and exclusion criteria.
Results: A total of 6 studies were included in this review. All studies were large population registries or cohort studies, which varied in transplant era, type of organ transplanted and immunosuppression protocol used. Overall, there was no clear difference demonstrated between tacrolimus and MPA in de novo PTM risk following solid organ transplantation. Furthermore, no study provided a direct comparison of carcinogenic risk between tacrolimus and MPA monotherapy in solid organ transplantation recipients.
Conclusion: The contrasting carcinogenic risk profiles of tacrolimus and MPA demonstrated in previous experimental studies, and its application in solid organ transplantation, is yet to be confirmed in clinical studies. Thus, the optimal choice of immunosuppression drug to use as maintenance monotherapy in LT recipients is not supported by a strong evidence base and remains unclear.
Keywords: Carcinogenicity; Immunosuppression; Liver transplantation; Mycophenolate; Solid organ transplantation; Tacrolimus.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to report.
Figures
Similar articles
-
Clinical pharmacokinetics and pharmacodynamics of mycophenolate in solid organ transplant recipients.Clin Pharmacokinet. 2007;46(1):13-58. doi: 10.2165/00003088-200746010-00002. Clin Pharmacokinet. 2007. PMID: 17201457 Review.
-
Comparison of the characteristics of adult liver transplant recipients with prope (almost) tolerance and full immunosuppression regimen.Transpl Immunol. 2021 Oct;68:101440. doi: 10.1016/j.trim.2021.101440. Epub 2021 Jul 31. Transpl Immunol. 2021. PMID: 34343659
-
Immunosuppression management in renal transplant recipients with normal-immunological risk: 10-year results from the Swiss Transplant Cohort Study.Swiss Med Wkly. 2020 Dec 5;150:w20354. doi: 10.4414/smw.2020.20354. eCollection 2020 Nov 30. Swiss Med Wkly. 2020. PMID: 33277913 Clinical Trial.
-
An open-label, randomized trial indicates that everolimus with tacrolimus or cyclosporine is comparable to standard immunosuppression in de novo kidney transplant patients.Kidney Int. 2019 Jul;96(1):231-244. doi: 10.1016/j.kint.2019.01.041. Epub 2019 Feb 27. Kidney Int. 2019. PMID: 31027892 Clinical Trial.
-
Calcineurin inhibitor-free immunosuppression in pediatric renal transplantation: a viable option?Paediatr Drugs. 2011 Feb 1;13(1):49-69. doi: 10.2165/11538530-000000000-00000. Paediatr Drugs. 2011. PMID: 21162600 Review.
Cited by
-
Factors influencing intrapatient variability of tacrolimus and its association with 1-year post-transplant outcomes in pediatric liver transplant recipients.Front Pharmacol. 2024 Nov 21;15:1473891. doi: 10.3389/fphar.2024.1473891. eCollection 2024. Front Pharmacol. 2024. PMID: 39640481 Free PMC article.
References
-
- McCaughan GW, Munn SR. Liver transplantation in Australia and New Zealand. Liver Transpl. 2016;22:830–838. - PubMed
-
- Herrero JI. De novo malignancies following liver transplantation: impact and recommendations. Liver Transpl. 2009;15 Suppl 2:S90–S94. - PubMed
-
- Gelson W, Hoare M, Dawwas MF, Vowler S, Gibbs P, Alexander G. The pattern of late mortality in liver transplant recipients in the United Kingdom. Transplantation. 2011;91:1240–1244. - PubMed
-
- Chandok N, Watt KD. Burden of de novo malignancy in the liver transplant recipient. Liver Transpl. 2012;18:1277–1289. - PubMed
LinkOut - more resources
Full Text Sources
