

Physiological changes after fluid bolus therapy in cardiac surgery patients: A propensity score matched case-control study
- PMID: 38690188
- PMCID: PMC11056405
- DOI: 10.1016/j.ccrj.2023.11.005
Physiological changes after fluid bolus therapy in cardiac surgery patients: A propensity score matched case-control study
Abstract
Objective: Fluid bolus therapy (FBT) is ubiquitous in intensive care units (ICUs) after cardiac surgery. However, its physiological effects remain unclear.
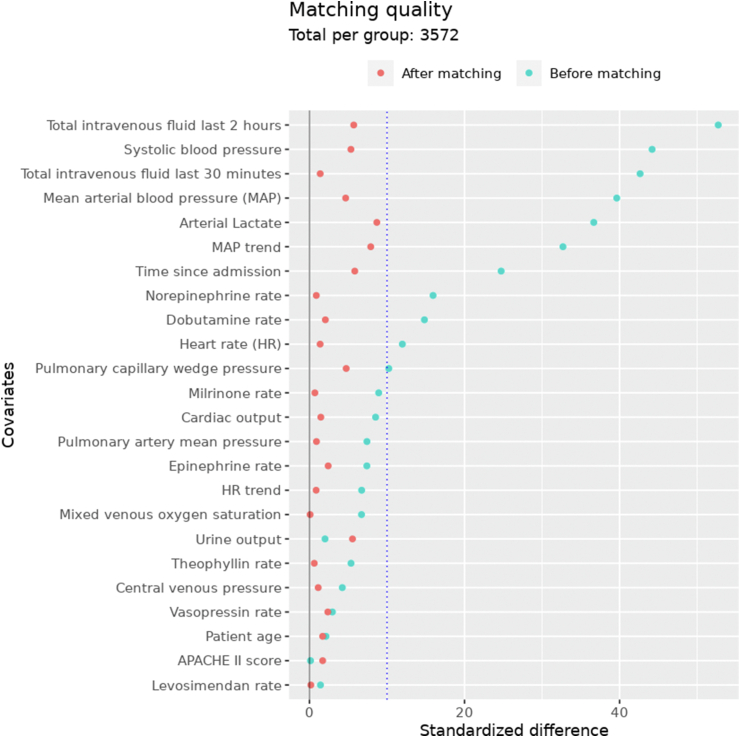
Design: : We performed an electronic health record-based quasi-experimental ICU study after cardiac surgery. We applied propensity score matching and compared the physiological changes after FBT episodes to matched control episodes where despite equivalent physiology no fluid bolus was given.
Setting: The study was conducted in a multidisciplinary ICU of a tertiary-level academic hospital.
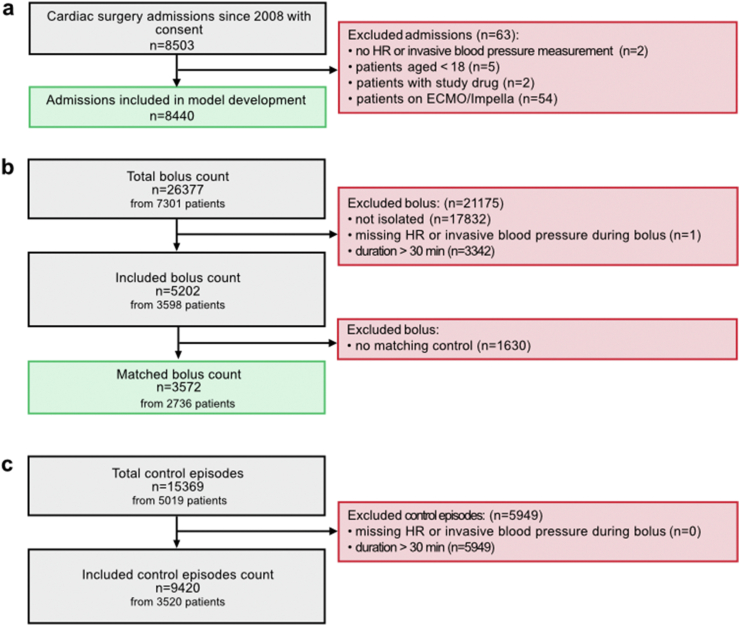
Participants: The study included 2,736 patients who underwent Coronary Artery Bypass Grafting and/or heart valve surgery.
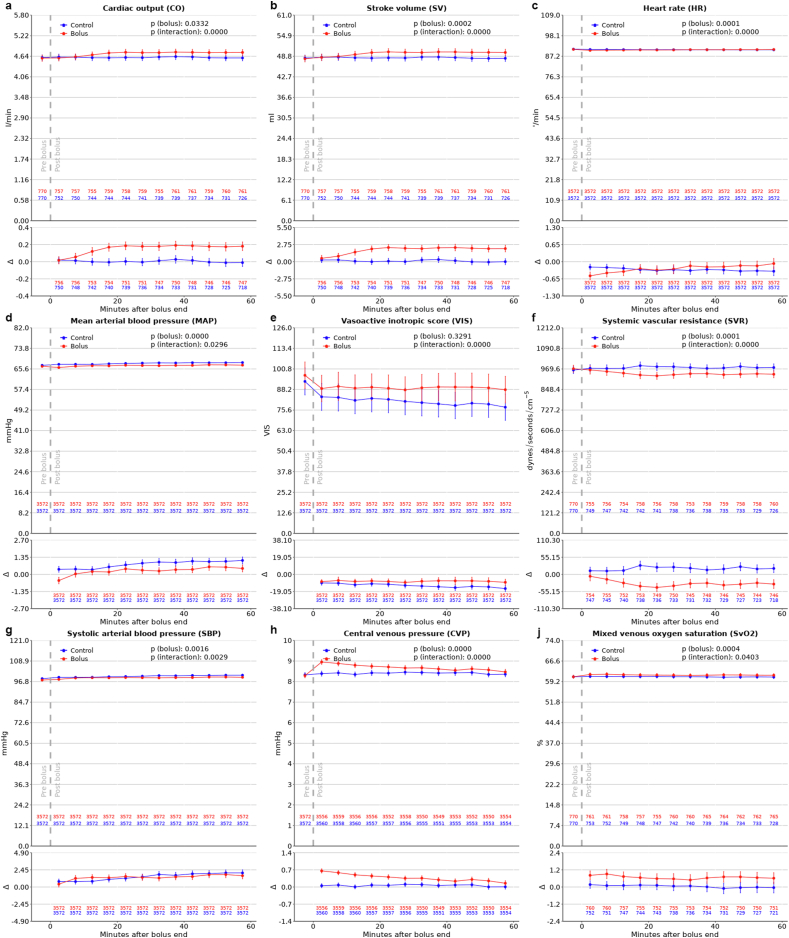
Main outcome measures: Changes in cardiac output (CO) and mean arterial pressure (MAP) during the 60 minutes following FBT.
Results: We analysed 3572 matched fluid bolus (FB) episodes. After FBT, but not in control episodes, CO increased within 10 min, with a maximum increase of 0.2 l/min (95%CI 0.1 to 0.2) or 4% above baseline at 40 min (p < 0.0001 vs. controls). CO increased by > 10% from baseline in 60.6% of FBT and 49.1% of control episodes (p < 0.0001). MAP increased by > 10% in 51.7% of FB episodes compared to 53.4% of controls. Finally, FBT was not associated with changes in acid-base status or oxygen delivery.
Conclusion: In this quasi-experimental comparative ICU study in cardiac surgery patients, FBT was associated with statistically significant but numerically small increases in CO. Nearly half of FBT failed to induce a positive CO or MAP response.
Keywords: Cardiac surgery; Hypotension; Intensive care; Resuscitation.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Gelbart B., Glassford N.J., Bellomo R. Fluid bolus therapy-based resuscitation for severe sepsis in hospitalized children: a systematic review. Pediatr Crit Care Med. 2015 Oct;16(8):e297–e307. - PubMed
-
- Jardin F., Fourme T., Page B., Loubières Y., Vieillard-Baron A., Beauchet A., et al. Persistent preload defect in severe sepsis despite fluid loading: a longitudinal echocardiographic study in patients with septic shock. Chest. 1999 Nov;116(5):1354–1359. - PubMed
-
- Glassford N.J., Mårtensson J., Eastwood G.M., Jones S.L., Tanaka A., Wilkman E., et al. Defining the characteristics and expectations of fluid bolus therapy: a worldwide perspective. J Crit Care. 2016 Oct;35:126–132. - PubMed
