

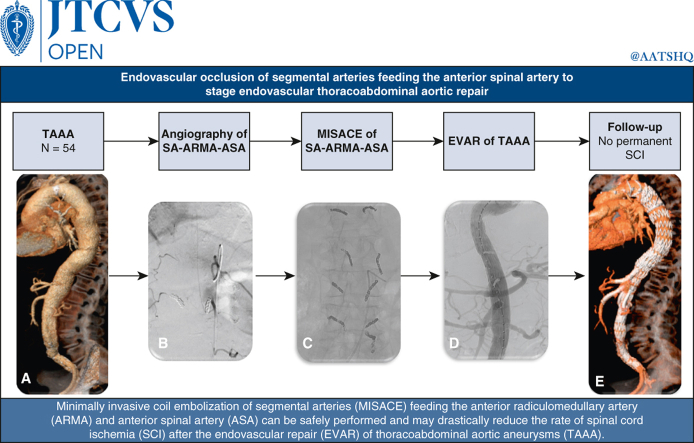
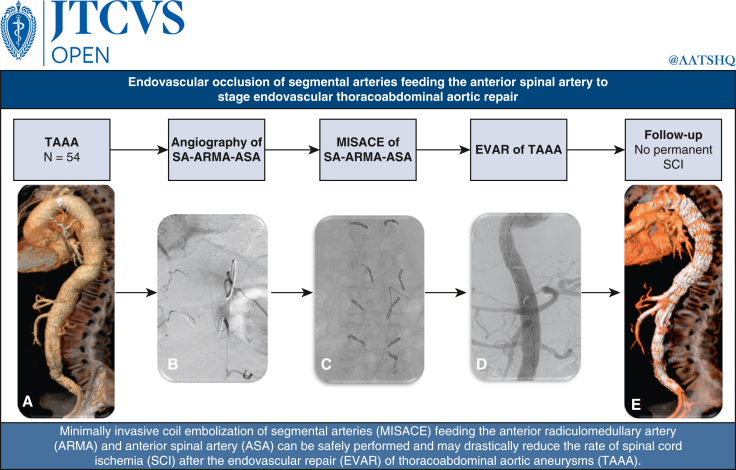
Endovascular occlusion of segmental arteries feeding the anterior spinal artery to stage endovascular thoracoabdominal aortic repair
- PMID: 38690411
- PMCID: PMC11056496
- DOI: 10.1016/j.xjon.2024.02.016
Endovascular occlusion of segmental arteries feeding the anterior spinal artery to stage endovascular thoracoabdominal aortic repair
Abstract
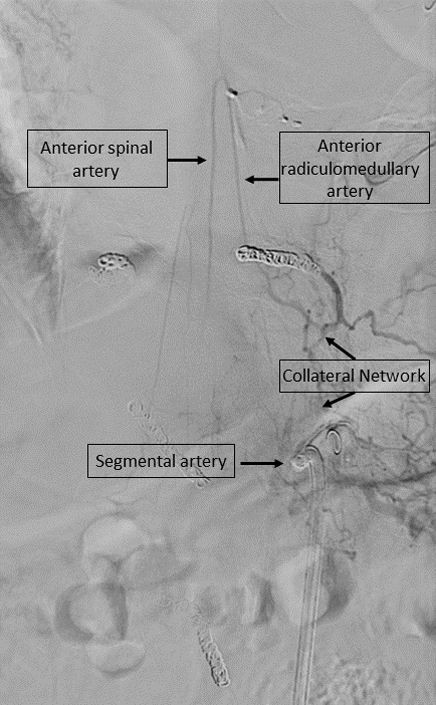
Objective: Minimally invasive segmental artery coil embolization was introduced to prevent spinal cord ischemia after endovascular repair of thoracoabdominal aortic aneurysms. There is no consensus on whether the endovascular occlusion of segmental arteries feeding directly the anterior radiculomedullary artery and anterior spinal artery can be safely performed without causing spinal cord ischemia. Our aim was to investigate the feasibility and clinical impact of endovascular occlusion of segmental arteries supplying the anterior spinal artery during minimally invasive segmental artery coil embolization in patients with thoracoabdominal aortic aneurysms.
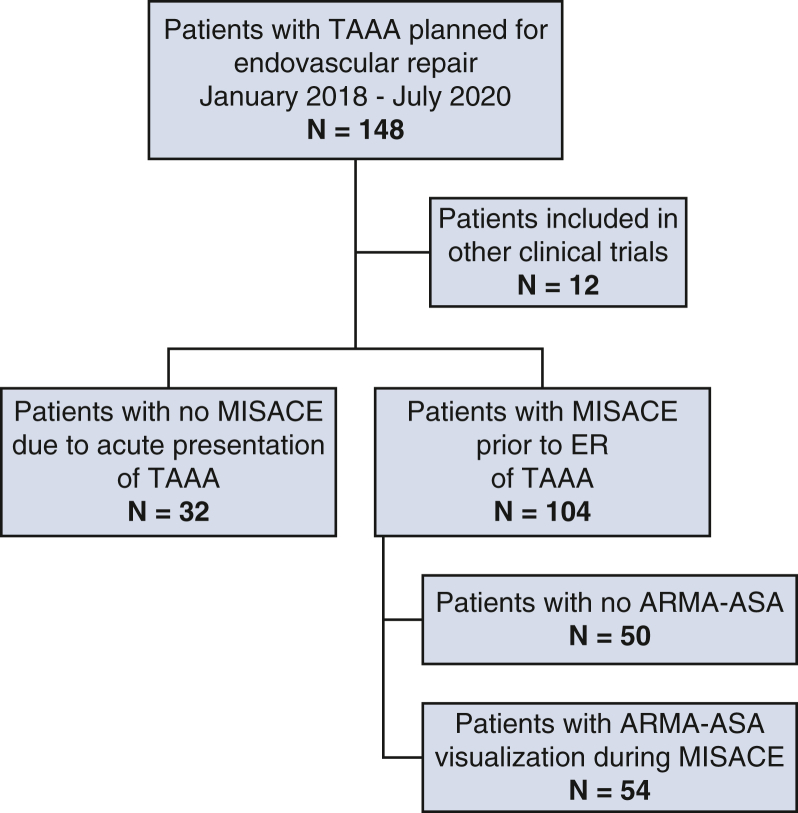
Methods: Between January 2018 and July 2020, 54 patients (36 male; mean age, 71.1 ± 9.3 years) underwent direct embolization of segmental arteries feeding the anterior radiculomedullary artery before endovascular repair of thoracoabdominal aortic aneurysms. End points included technical success of minimally invasive segmental artery coil embolization of segmental arteries, anterior radiculomedullary artery, neurological complications, and in-hospital mortality after minimally invasive segmental artery coil embolization and endovascular repair of thoracoabdominal aortic aneurysms.
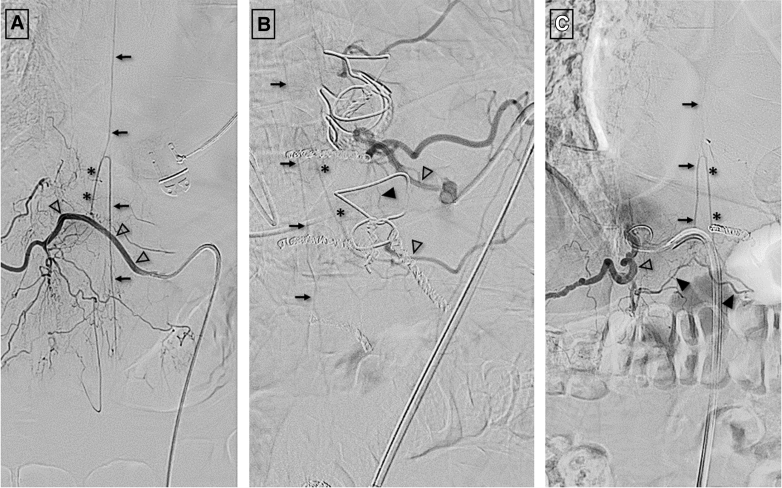
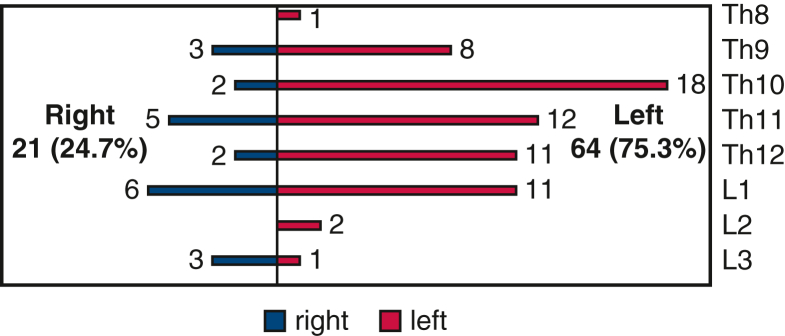
Results: The thoracoabdominal aortic aneurysm classification was type I (n = 8), type II (n = 24), type III (n = 11), and type IV (n = 11). During minimally invasive segmental artery coil embolization, 388 segmental arteries were occluded, each patient having 7.2 ± 3.1 coiled segmental arteries occluding 64.5% (25-100%) of open segmental arteries within the treated aortic segment. Altogether, 66 anterior radiculomedullary arteries were seen originating between Th8 and L3 levels from 85 (21.9%) segmental arteries. In 10 patients (18.5%), 2 large anterior radiculomedullary arteries were identified, and 1 patient (1.9%) showed 3 anterior radiculomedullary arteries on the spinal arteriography. No spinal cord ischemia or procedure-related complications occurred after minimally invasive segmental artery coil embolization. After 47.9 ± 39.4 days, all patients received endovascular repair of their thoracoabdominal aortic aneurysms. There was no in-hospital mortality. One male patient developed incomplete temporary spinal cord ischemia after endovascular repair.
Conclusions: Minimally invasive segmental artery coil embolization of segmental arteries feeding the anterior spinal artery in patients with thoracoabdominal aortic aneurysms to prevent spinal cord ischemia after endovascular repair is feasible and clinically safe.
Keywords: coil embolization; great anterior radiculomedullary artery; segmental artery; spinal cord ischemia; thoracoabdominal aortic aneurysm.
© 2024 The Author(s).
Conflict of interest statement
D.B.: grants: Artivion, Bentley Innomed, COOK Medical, Endologix, Getinge, Medtronic. S.S.: speakers' honorarium: Bayer Medical, research funding: C.R. Bard. D.S.: consultant or advisory board member for Abbott, Biotronik, Boston Scientific, Cook Medical, Cordis, BD, Gardia Medical, Medtronic, TriReme Medical, and Upstream Peripheral Technologies. A.S.: Consulting/speakers honorarium: Abbott Vascular, BD, Boston Scientific, Cook, Cardinal Health/Cordis, Phillips, and Upstream Peripheral. All other authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures
Similar articles
-
First-in-man endovascular preconditioning of the paraspinal collateral network by segmental artery coil embolization to prevent ischemic spinal cord injury.J Thorac Cardiovasc Surg. 2015 Apr;149(4):1074-9. doi: 10.1016/j.jtcvs.2014.12.025. Epub 2014 Dec 18. J Thorac Cardiovasc Surg. 2015. PMID: 25906717
-
Minimally invasive segmental artery coil embolization for preconditioning of the spinal cord collateral network before one-stage descending and thoracoabdominal aneurysm repair.Innovations (Phila). 2014 Jan-Feb;9(1):60-5. doi: 10.1097/IMI.0000000000000038. Innovations (Phila). 2014. PMID: 24476953
-
Minimally Invasive Segmental Artery Coil Embolization (MISACE) Prior to Endovascular Thoracoabdominal Aortic Aneurysm Repair.Cardiovasc Intervent Radiol. 2022 Oct;45(10):1462-1469. doi: 10.1007/s00270-022-03230-y. Epub 2022 Aug 4. Cardiovasc Intervent Radiol. 2022. PMID: 35927497
-
Comparison of single- and multistage strategies during fenestrated-branched endovascular aortic repair of thoracoabdominal aortic aneurysms.J Vasc Surg. 2023 Jun;77(6):1588-1597.e4. doi: 10.1016/j.jvs.2023.01.188. Epub 2023 Jan 31. J Vasc Surg. 2023. PMID: 36731757 Review.
-
The Safety and Outcome of Minimally Invasive Staged Segmental Artery Coil Embolization (MIS2ACE) Prior Thoracoabdominal Aortic Aneurysm Repair: A Single-Center Study, Systematic Review, and Meta-Analysis.J Clin Med. 2024 Feb 29;13(5):1408. doi: 10.3390/jcm13051408. J Clin Med. 2024. PMID: 38592242 Free PMC article. Review.
References
-
- Riambau V., Böckler D., Brunkwall J., et al. Editor's choice - management of descending thoracic aorta diseases: clinical practice guidelines of the European Society for Vascular Surgery (ESVS) Eur J Vasc Endovasc Surg. 2017;53:4–52. - PubMed
-
- Greenberg R.K., Lu Q., Roselli E.E., et al. Contemporary analysis of descending thoracic and thoracoabdominal aneurysm repair: a comparison of endovascular and open techniques. Circulation. 2008;118:808–817. - PubMed
-
- Katsargyris A., Oikonomou K., Kouvelos G., Renner H., Ritter W., Verhoeven E.L.G. Spinal cord ischemia after endovascular repair of thoracoabdominal aortic aneurysms with fenestrated and branched stent grafts. J Vasc Surg. 2015;62:1450–1456. - PubMed
-
- Maurel B., Delclaux N., Sobocinski J., et al. The impact of early pelvic and lower limb reperfusion and attentive peri-operative management on the incidence of spinal cord ischemia during thoracoabdominal aortic aneurysm endovascular repair. Eur J Vasc Endovasc Surg. 2015;49:248–254. - PubMed
-
- Cheng D., Martin J., Shennib H., et al. Endovascular aortic repair versus open surgical repair for descending thoracic aortic disease a systematic review and meta-analysis of comparative studies. J Am Coll Cardiol. 2010;55:986–1001. - PubMed
LinkOut - more resources
Full Text Sources
