

Evidence of the existence of multiple modules for the stroke-caused flexion synergy from Fugl-Meyer assessment scores
- PMID: 38691520
- PMCID: PMC11381114
- DOI: 10.1152/jn.00067.2024
Evidence of the existence of multiple modules for the stroke-caused flexion synergy from Fugl-Meyer assessment scores
Abstract
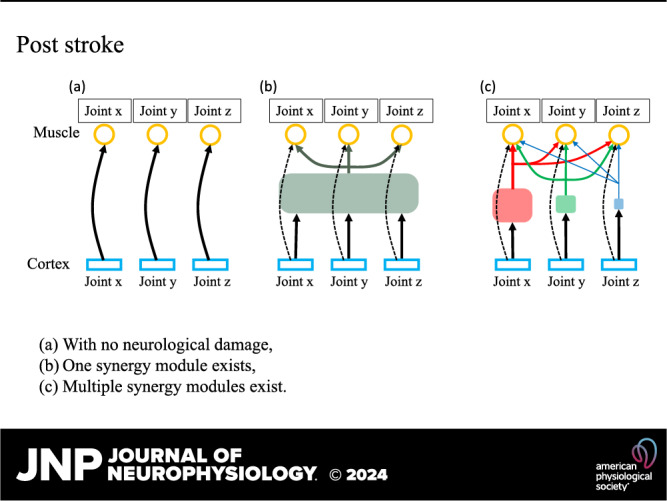
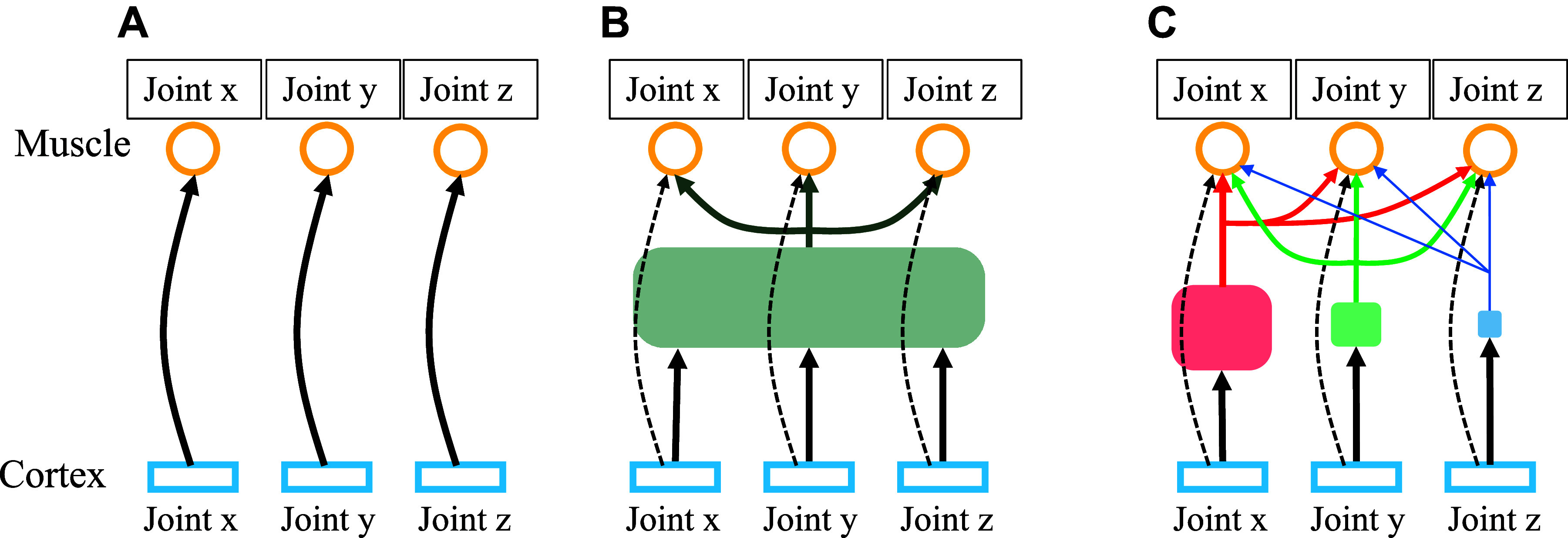
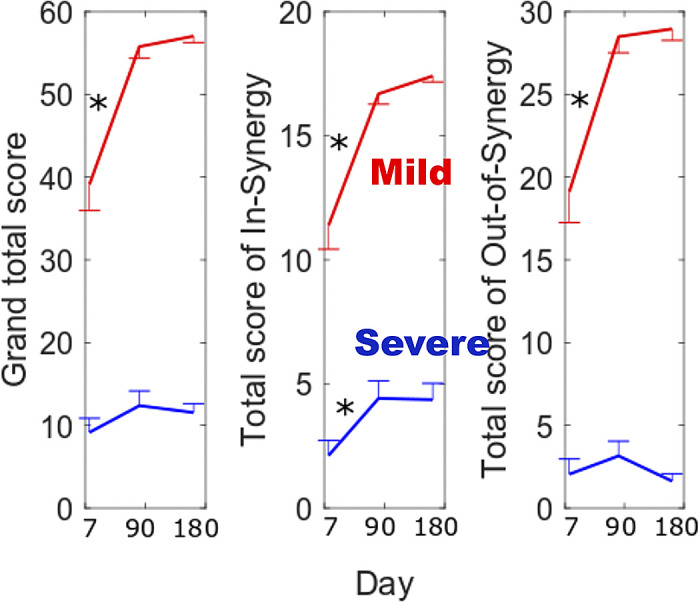
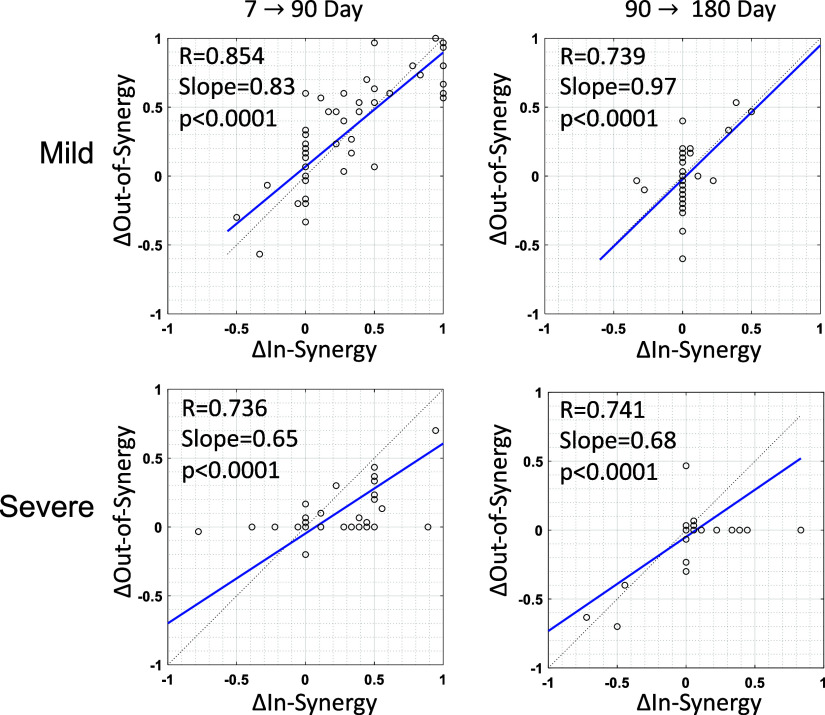
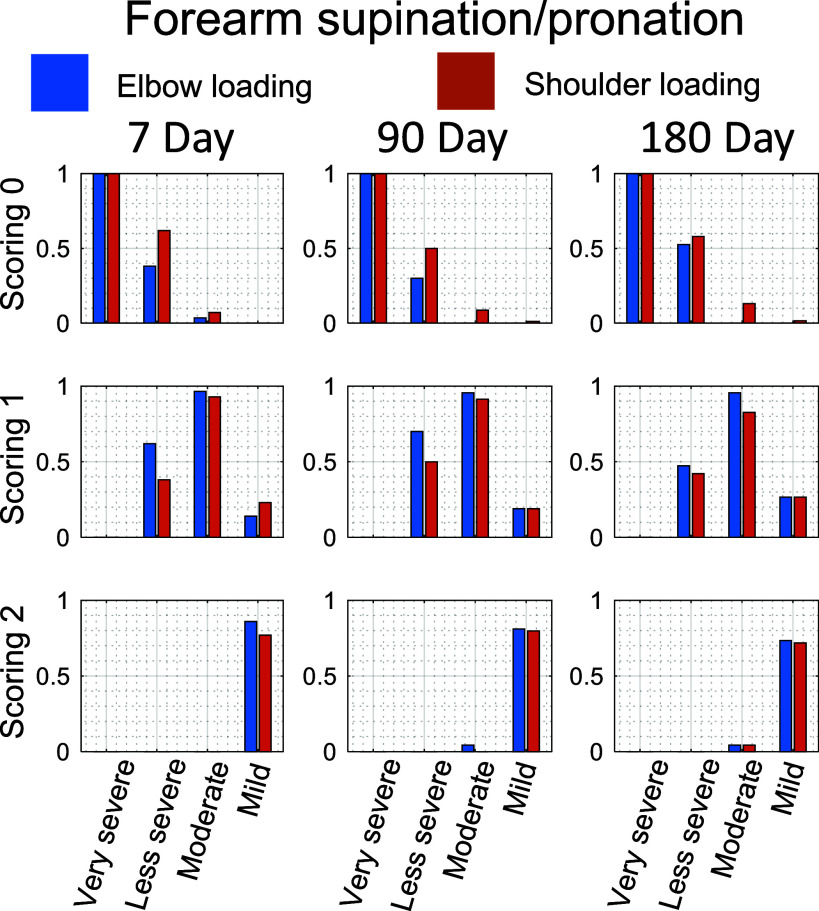
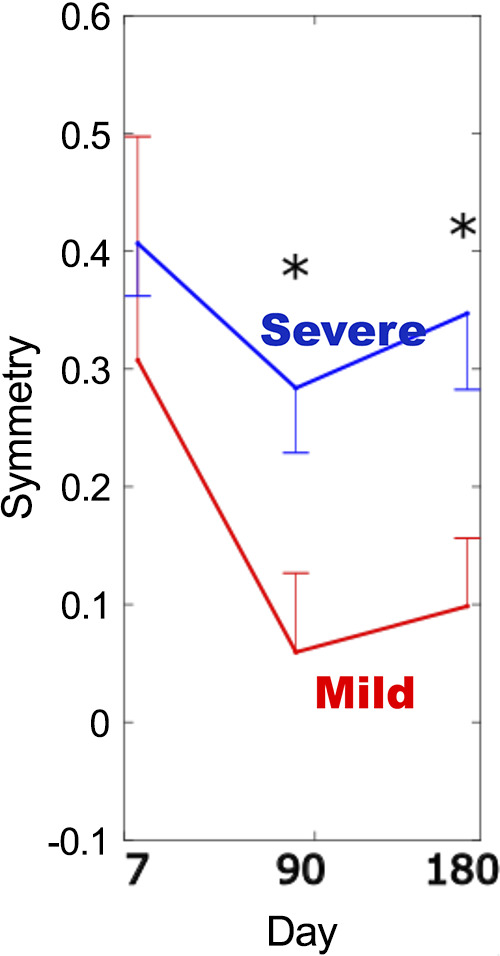
Stroke-caused synergies may result from the preferential use of the reticulospinal tract (RST) due to damage to the corticospinal tract. The RST branches multiple motoneuron pools across the arm together resulting in gross motor control or abnormal synergies, and accordingly, the controllability of individual muscles decreases. However, it is not clear whether muscles involuntarily activated by abnormal synergy vary depending on the muscles voluntarily activated when motor commands descend through the RST. Studies showed that abnormal synergies may originate from the merging and reweighting of synergies in individuals without neurological deficits. This leads to a hypothesis that those abnormal synergies are still selectively excited depending on the context. In this study, we test this hypothesis, leveraging the Fugl-Meyer assessment that could characterize the neuroanatomical architecture in individuals with a wide range of impairments. We examine the ability to perform an out-of-synergy movement with the flexion synergy caused by either shoulder or elbow loading. The results reveal that about 14% [8/57, 95% confidence interval (5.0%, 23.1%)] of the participants with severe impairment (total Fugl-Meyer score <29) in the chronic phase (6 months after stroke) are able to keep the elbow extended during shoulder loading and keep the shoulder at neutral during elbow loading. Those participants underwent a different course of neural reorganization, which enhanced abnormal synergies in comparison with individuals with mild impairment (P < 0.05). These results provide evidence that separate routes and synergy modules to motoneuron pools across the arm might exist even if the motor command is mediated possibly via the RST.NEW & NOTEWORTHY We demonstrate that abnormal synergies are still selectively excited depending on the context.
Keywords: abnormal synergies; reticulospinal tract; stroke; synergy module.
Conflict of interest statement
The authors declare no competing financial and/or nonfinancial interests in relation to the work described. Dongwon Kim declares the ownership of EpicWide, LLC.
Figures
Similar articles
-
Lumbar sympathectomy versus prostanoids for critical limb ischaemia due to non-reconstructable peripheral arterial disease.Cochrane Database Syst Rev. 2018 Apr 16;4(4):CD009366. doi: 10.1002/14651858.CD009366.pub2. Cochrane Database Syst Rev. 2018. PMID: 29658630 Free PMC article.
-
Incentives for preventing smoking in children and adolescents.Cochrane Database Syst Rev. 2017 Jun 6;6(6):CD008645. doi: 10.1002/14651858.CD008645.pub3. Cochrane Database Syst Rev. 2017. PMID: 28585288 Free PMC article.
-
Identifying alterations in hand movement coordination from chronic stroke survivors using a wearable high-density EMG sleeve.J Neural Eng. 2024 Aug 5;21(4). doi: 10.1088/1741-2552/ad634d. J Neural Eng. 2024. PMID: 39008975
-
Antiemetics for adults for prevention of nausea and vomiting caused by moderately or highly emetogenic chemotherapy: a network meta-analysis.Cochrane Database Syst Rev. 2021 Nov 16;11(11):CD012775. doi: 10.1002/14651858.CD012775.pub2. Cochrane Database Syst Rev. 2021. PMID: 34784425 Free PMC article.
-
Automated monitoring compared to standard care for the early detection of sepsis in critically ill patients.Cochrane Database Syst Rev. 2018 Jun 25;6(6):CD012404. doi: 10.1002/14651858.CD012404.pub2. Cochrane Database Syst Rev. 2018. PMID: 29938790 Free PMC article.
Cited by
-
Insights into the dependence of post-stroke motor recovery on the initial corticospinal tract connectivity from a computational model.J Neuroeng Rehabil. 2025 Jan 20;22(1):8. doi: 10.1186/s12984-024-01513-8. J Neuroeng Rehabil. 2025. PMID: 39833900 Free PMC article.
References
-
- Ellis MD, Lan Y, Yao J, Dewald JP. Robotic quantification of upper extremity loss of independent joint control or flexion synergy in individuals with hemiparetic stroke: a review of paradigms addressing the effects of shoulder abduction loading. J Neuroeng Rehabil 13: 95, 2016. doi: 10.1186/s12984-016-0203-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical