

Impact of left atrial appendage flow velocity on thrombus resolution and clinical outcomes in patients with atrial fibrillation and silent left atrial thrombi: insights from the LAT study
- PMID: 38691672
- PMCID: PMC11106584
- DOI: 10.1093/europace/euae120
Impact of left atrial appendage flow velocity on thrombus resolution and clinical outcomes in patients with atrial fibrillation and silent left atrial thrombi: insights from the LAT study
Abstract
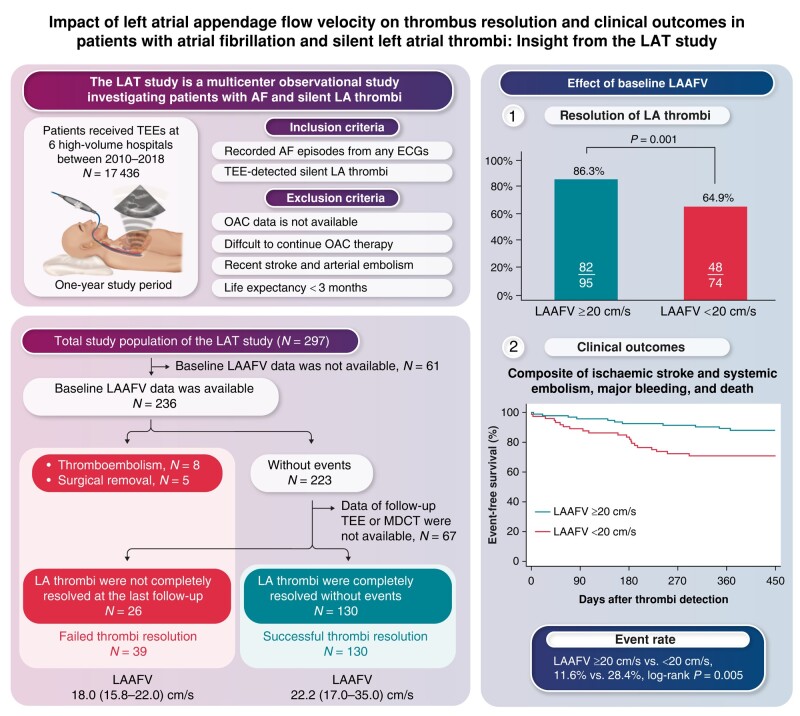
Aims: Blood stasis is crucial in developing left atrial (LA) thrombi. LA appendage peak flow velocity (LAAFV) is a quantitative parameter for estimating thromboembolic risk. However, its impact on LA thrombus resolution and clinical outcomes remains unclear.
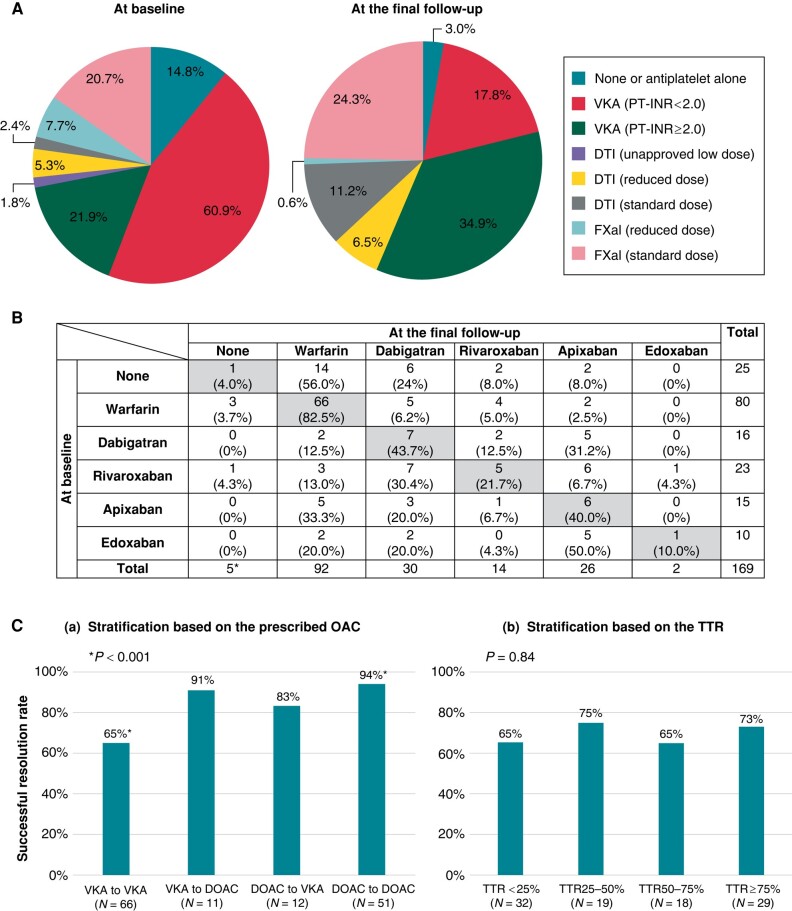
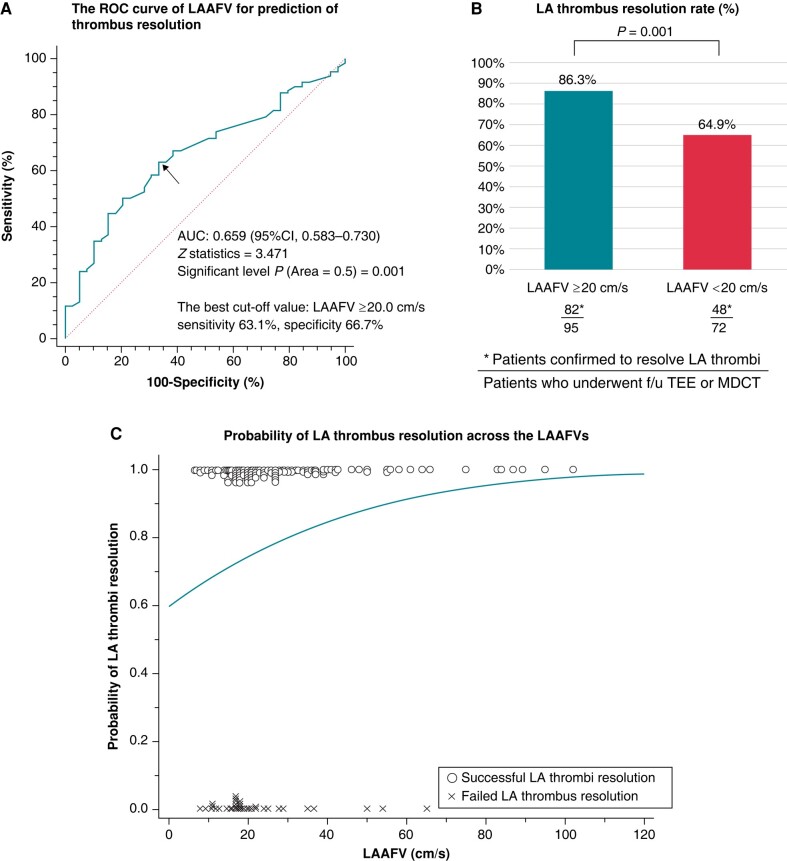
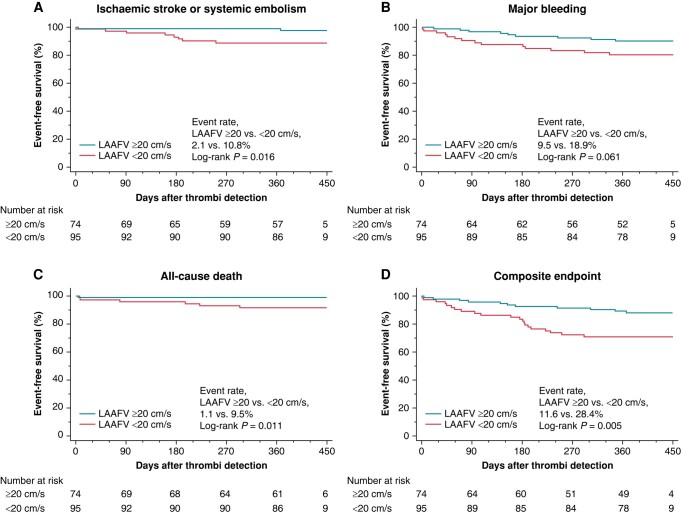
Methods and results: The LAT study was a multicentre observational study investigating patients with atrial fibrillation (AF) and silent LA thrombi detected by transoesophageal echocardiography (TEE). Among 17 436 TEE procedures for patients with AF, 297 patients (1.7%) had silent LA thrombi. Excluding patients without follow-up examinations, we enrolled 169 whose baseline LAAFV was available. Oral anticoagulation use increased from 85.7% at baseline to 97.0% at the final follow-up (P < 0.001). During 1 year, LA thrombus resolution was confirmed in 130 (76.9%) patients within 76 (34-138) days. Conversely, 26 had residual LA thrombi, 8 had thromboembolisms, and 5 required surgical removal. These patients with failed thrombus resolution had lower baseline LAAFV than those with successful resolution (18.0 [15.8-22.0] vs. 22.2 [17.0-35.0], P = 0.003). Despite limited predictive power (area under the curve, 0.659; P = 0.001), LAAFV ≤ 20.0 cm/s (best cut-off) significantly predicted failed LA thrombus resolution, even after adjusting for potential confounders (odds ratio, 2.72; 95% confidence interval, 1.22-6.09; P = 0.015). The incidence of adverse outcomes including ischaemic stroke/systemic embolism, major bleeding, or all-cause death was significantly higher in patients with reduced LAAFV than in those with preserved LAAFV (28.4% vs. 11.6%, log-rank P = 0.005).
Conclusion: Failed LA thrombus resolution was not rare in patients with AF and silent LA thrombi. Reduced LAAFV was associated with failed LA thrombus resolution and adverse clinical outcomes.
Keywords: Atrial fibrillation; Left atrial appendage flow velocity; Left atrial thrombus; Oral anticoagulant; Transesophageal echocardiography.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures


Similar articles
-
Morphology and location of thrombus and sludge in patients with non-valvular atrial fibrillation.BMC Cardiovasc Disord. 2024 Jul 31;24(1):398. doi: 10.1186/s12872-024-04073-w. BMC Cardiovasc Disord. 2024. PMID: 39085776 Free PMC article.
-
Left atrial thrombus in patients with atrial fibrillation and under oral anticoagulant therapy; 3-D transesophageal echocardiographic study.Int J Cardiovasc Imaging. 2020 Jun;36(6):1097-1103. doi: 10.1007/s10554-020-01811-x. Epub 2020 Mar 5. Int J Cardiovasc Imaging. 2020. PMID: 32140812
-
Use of transesophageal contrast echocardiography for excluding left atrial appendage thrombi in patients with atrial fibrillation before cardioversion.J Am Soc Echocardiogr. 2002 Oct;15(10 Pt 2):1256-61. doi: 10.1067/mje.2002.123961. J Am Soc Echocardiogr. 2002. PMID: 12411914
-
Overcoming barriers for left atrial appendage thrombus: a systematic review of left atrial appendage closure.BMC Cardiovasc Disord. 2024 Mar 21;24(1):175. doi: 10.1186/s12872-024-03843-w. BMC Cardiovasc Disord. 2024. PMID: 38515032 Free PMC article.
-
Review of the Etiology, Diagnosis, and Therapy of Left Atrial Thrombus.Cardiol Rev. 2025 Mar-Apr 01;33(2):135-138. doi: 10.1097/CRD.0000000000000592. Epub 2023 Aug 2. Cardiol Rev. 2025. PMID: 37530541 Review.
Cited by
-
Comparison between DOACs and warfarin for left atrial thrombus in atrial fibrillation patients.Int J Cardiol Heart Vasc. 2025 Jul 8;59:101745. doi: 10.1016/j.ijcha.2025.101745. eCollection 2025 Aug. Int J Cardiol Heart Vasc. 2025. PMID: 40687395 Free PMC article.
References
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991;22:983–8. - PubMed
-
- Watson T, Shantsila E, Lip GY. Mechanisms of thrombogenesis in atrial fibrillation: virchow’s triad revisited. Lancet 2009;373:155–66. - PubMed
-
- Ding WY, Gupta D, Lip GYH. Atrial fibrillation and the prothrombotic state: revisiting Virchow’s triad in 2020. Heart 2020;106:1463–8. - PubMed
-
- Zhan Y, Joza J, Al Rawahi M, Barbosa RS, Samuel M, Bernier M et al. Assessment and management of the left atrial appendage thrombus in patients with nonvalvular atrial fibrillation. Can J Cardiol 2018;34:252–61. - PubMed
-
- Lurie A, Wang J, Hinnegan KJ, McIntyre WF, Belley-Côté EP, Amit G et al. Prevalence of left atrial thrombus in anticoagulated patients with atrial fibrillation. J Am Coll Cardiol 2021;77:2875–86. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
