

Association of GLP-1 Receptor Agonists and Hepatocellular Carcinoma Incidence and Hepatic Decompensation in Patients With Type 2 Diabetes
- PMID: 38692395
- PMCID: PMC12294230
- DOI: 10.1053/j.gastro.2024.04.029
Association of GLP-1 Receptor Agonists and Hepatocellular Carcinoma Incidence and Hepatic Decompensation in Patients With Type 2 Diabetes
Abstract
Background & aims: Hepatocellular carcinoma (HCC) is a leading cause of cancer death. HCC is preventable with about 70% of HCC attributable to modifiable risk factors. Glucagon-like peptide-1 receptor agonists (GLP-1RAs), Food and Drug Administration-approved medications for treating type 2 diabetes mellitus (T2DM), have pleiotropic effects on counteracting risk factors for HCC. Here we evaluate the association of GLP-1RAs with incident HCC risk in a real-world population.
Methods: This retrospective cohort included 1,890,020 patients with a diagnosis of T2DM who were prescribed GLP-1RAs or other non-GLP-1RA anti-diabetes medications and had no prior diagnosis of HCC. Incident (first-time) diagnosis of HCC and hepatic decompensating events during a 5-year follow-up was compared between cohorts of patients prescribed GLP-1 RAs vs other anti-diabetes medications. Time-to-first-event analysis was performed using Kaplan-Meier survival analysis with hazard ratio and 95% confidence interval calculated.
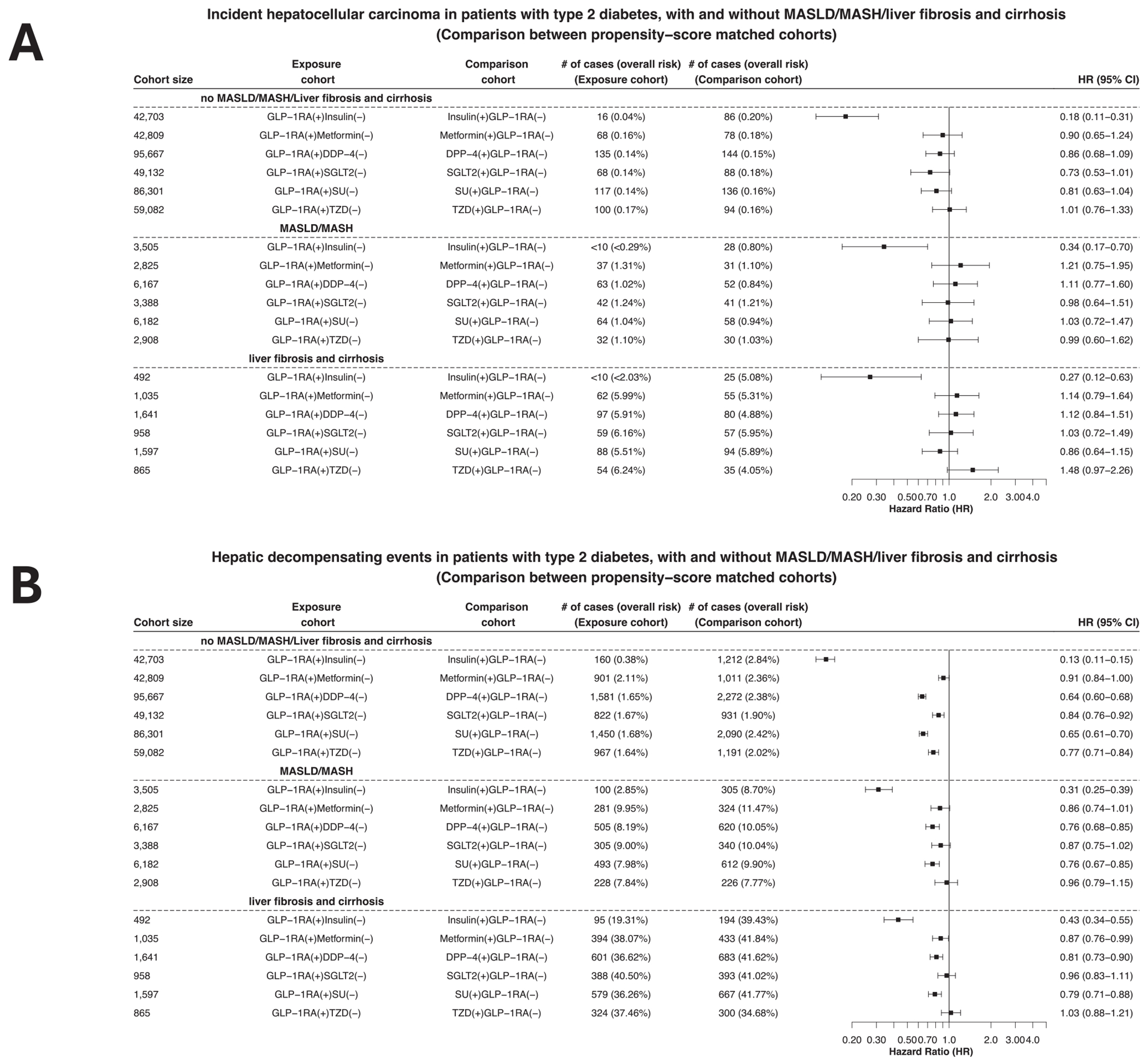
Results: GLP-1RAs were associated with a lower risk of incident HCC with hazard ratio of 0.20 [0.14-0.31], 0.39 [0.21-0.69], 0.63 [0.26-1.50] compared with insulin, sulfonylureas, and metformin, respectively. GLP-1RAs were associated with a significantly lower risk of hepatic decompensation compared with 6 other anti-diabetes medications. Reduced risks were observed in patients without and with different stages of fatty liver diseases, with more profound effects in patients without liver diseases. Similar findings were observed in patients with and without obesity and alcohol or tobacco use disorders. GLP-1RA combination therapies were associated with decreased risk for HCC and hepatic decompensations compared with monotherapies.
Conclusions: GLP-1RAs were associated with a reduced risk of incident HCC and hepatic decompensation compared with other anti-diabetes medications in patients with T2DM. These findings provide supporting evidence for future studies to investigate the underlying mechanisms and their clinical use.
Keywords: Cancer Prevention; Glucagon-Like Peptide-1 Receptor Agonists; Hepatocellular Carcinoma; Real-World Evidence; Type 2 Diabetes Mellitus.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
The authors disclose no conflicts.
Figures




References
-
- National Cancer Institute. Liver Cancer Causes, Risk Factors, and Prevention. Available at: https://www.cancer.gov/types/liver/what-is-liver-cancer/causes-risk-factors. Updated May 15, 2024.
-
- American Cancer Society. Cancer Facts & Figures 2023. Available at: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts.... Accessed November 6, 2023.
-
- Centers for Disease Control and Prevention. Liver Cancer Basics 2022. Available at: https://www.cdc.gov/cancer/liver/index.htm. Accessed November 2, 2023.
-
- Islami F, Goding Sauer A, Miller KD, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J Clin 2018;68:31–54. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
