

The Role of Obstructive Sleep Apnea in Hypercapnic Respiratory Failure Identified in Critical Care, Inpatient, and Outpatient Settings
- PMID: 38692757
- PMCID: PMC11068091
- DOI: 10.1016/j.jsmc.2024.02.012
The Role of Obstructive Sleep Apnea in Hypercapnic Respiratory Failure Identified in Critical Care, Inpatient, and Outpatient Settings
Abstract
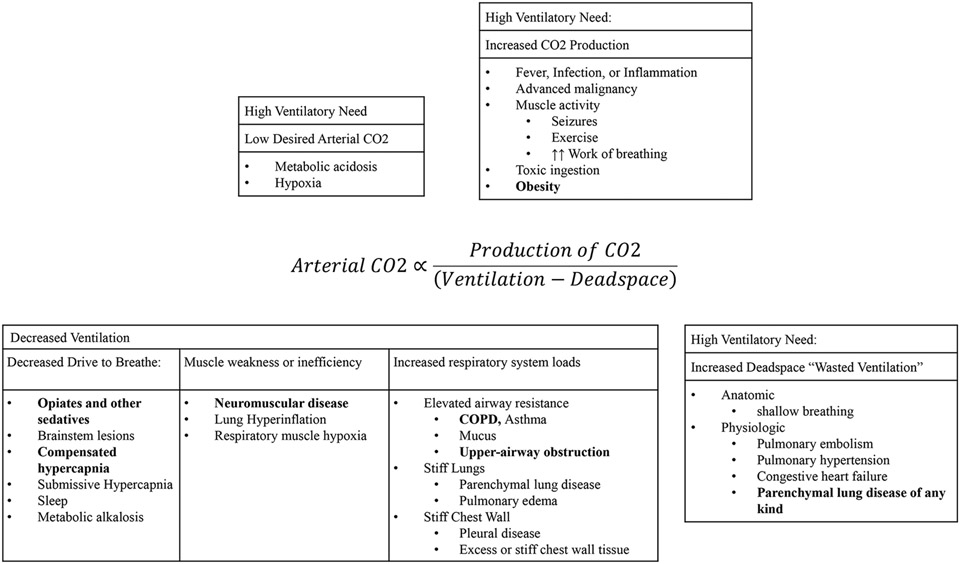
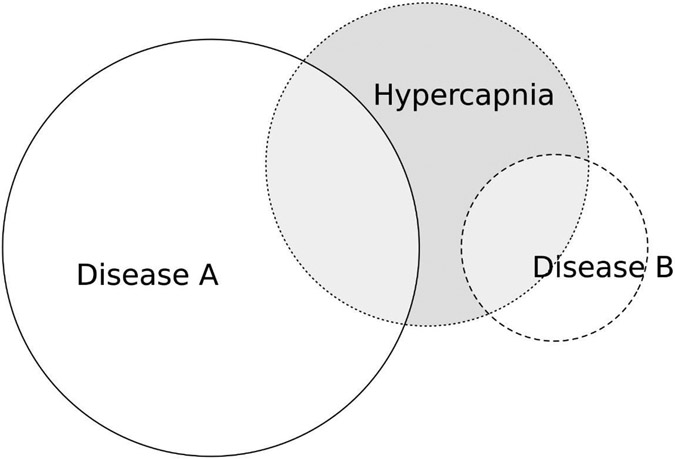
An emerging body of literature describes the prevalence and consequences of hypercapnic respiratory failure. While device qualifications, documentation practices, and previously performed clinical studies often encourage conceptualizing patients as having a single "cause" of hypercapnia, many patients encountered in practice have several contributing conditions. Physiologic and epidemiologic data suggest that sleep-disordered breathing-particularly obstructive sleep apnea (OSA)-often contributes to the development of hypercapnia. In this review, the authors summarize the frequency of contributing conditions to hypercapnic respiratory failure among patients identified in critical care, emergency, and inpatient settings with an aim toward understanding the contribution of OSA to the development of hypercapnia.
Keywords: Hypercapnia; Hypercapnic respiratory failure; Hypoventilation; Non-invasive ventilation; Positive airway pressure; Respiratory insufficiency; Sleep apnea.
Copyright © 2024 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure B.W. Locke. receives research funding from the American Thoracic Society ASPIRE Fellowship and the National Institutes of Health under the Ruth L. Kirschstein National Research Service Award 5T32HL105321 J.P. Brown. no conflicts of interest. K.M. Sundar is co-founder of Hypnoscure LLC—a software application for population management of sleep apnea through the University of Utah Technology Commercialization Office.
Figures
Similar articles
-
Sleep related respiratory events during non-invasive ventilation of patients with chronic hypoventilation.Respir Med. 2017 Nov;132:210-216. doi: 10.1016/j.rmed.2017.10.025. Epub 2017 Nov 2. Respir Med. 2017. PMID: 29229100
-
Non-invasive ventilation for obese patients with chronic respiratory failure: Are two pressures always better than one?Respirology. 2019 Oct;24(10):952-961. doi: 10.1111/resp.13588. Epub 2019 May 23. Respirology. 2019. PMID: 31121638 Review.
-
Real-life evaluation of NIV to CPAP switch in patients with chronic respiratory failure. A case control study.Respir Med Res. 2024 Nov;86:101114. doi: 10.1016/j.resmer.2024.101114. Epub 2024 May 2. Respir Med Res. 2024. PMID: 38875850
-
[Respiratory responses to CO2 stimulation in hypercapnic patients with obstructive sleep apnea syndrome].Pneumonol Alergol Pol. 2006;74(4):383-90. Pneumonol Alergol Pol. 2006. PMID: 17427147 Polish.
-
Supporting patients with hypercapnia.Clin Med (Lond). 2024 Jan;24(1):100007. doi: 10.1016/j.clinme.2023.100007. Epub 2024 Jan 18. Clin Med (Lond). 2024. PMID: 38382181 Free PMC article. Review.
Cited by
-
Association of the Neutrophil Percentage-to-Albumin Ratio with All-Cause Mortality in Patients with Hypercapnic Respiratory Failure: A Prospective Cohort Study.Int J Gen Med. 2025 Aug 12;18:4445-4456. doi: 10.2147/IJGM.S520510. eCollection 2025. Int J Gen Med. 2025. PMID: 40822899 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
