

Global hyperperfusion after successful endovascular thrombectomy is linked to worse outcome in acute ischemic stroke
- PMID: 38693311
- PMCID: PMC11063193
- DOI: 10.1038/s41598-024-60623-4
Global hyperperfusion after successful endovascular thrombectomy is linked to worse outcome in acute ischemic stroke
Abstract
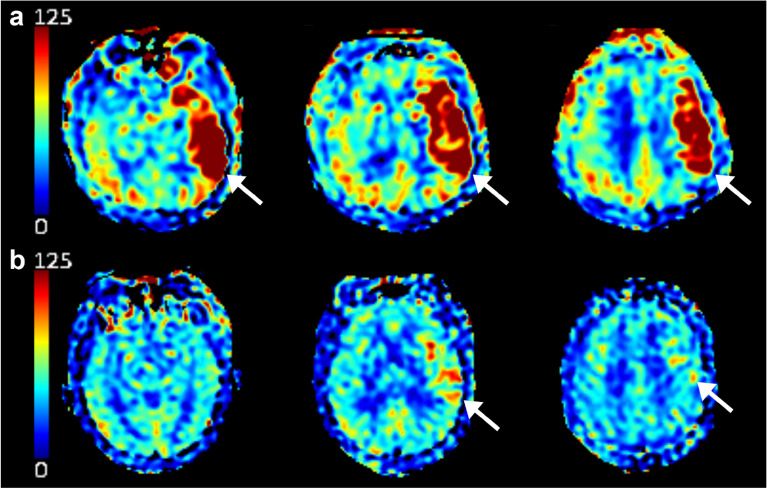
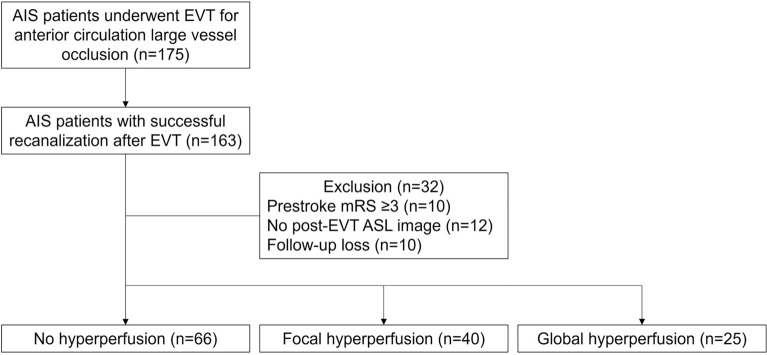
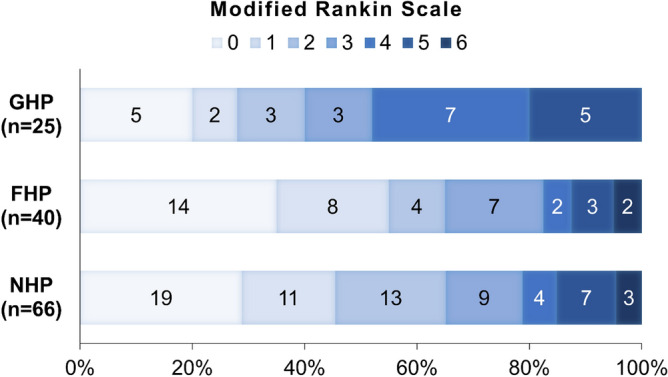
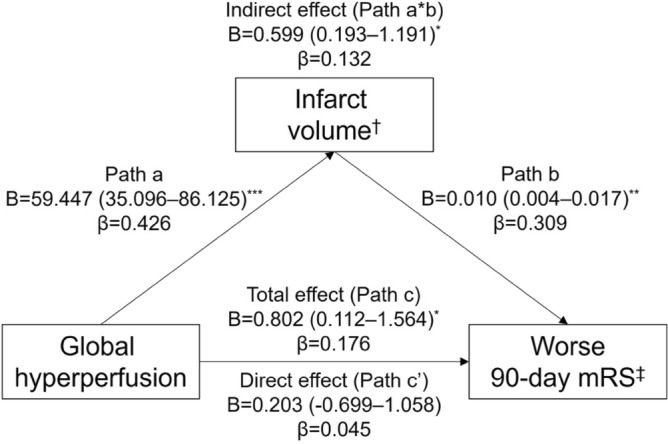
Patients with stroke may develop hyperperfusion after a successful endovascular thrombectomy (EVT). However, the relationship between post-EVT hyperperfusion and clinical outcomes remains unclear and requires further clarification. We reviewed consecutive patients with anterior circulation occlusion who were successfully recanalized with EVT. Based on post-EVT arterial spin-labeling images, hyperperfusion was categorized as follows: global hyperperfusion (GHP), increased cerebral blood flow (CBF) in ≥ 50% of the culprit vessel territory; focal hyperperfusion (FHP), increased CBF in < 50% of the culprit vessel territory; no hyperperfusion (NHP), no discernible CBF increase. Factors associated with hyperperfusion were assessed, and clinical outcomes were compared among patients under different hyperperfusion categories. Among 131 patients, 25 and 40 patients developed GHP and FHP, respectively. Compared to other groups, the GHP group had worse National Institutes of Health Stroke Scale score (GHP vs. NHP/FHP, 18.1 ± 7.4 vs. 12.3 ± 6.0; p < 0.001), a larger post-EVT infarct volume (98.9 [42.3-132.7] vs. 13.5 [5.0-34.1] mL; p < 0.001), and a worse 90-day outcome (modified Rankin Scale, 3 [1-4] vs. 2 [0-3]; p = 0.030). GHP was independently associated with infarct volume (B = 0.532, standard error = 0.163, p = 0.001), and infarct volume was a major mediator of the association of GHP with unfavorable outcomes (total effect: β = 0.176, p = 0.034; direct effect: β = 0.045, p = 0.64; indirect effect: β = 0.132, p = 0.017). Patients presenting with post-EVT GHP had poorer neurological prognosis, which is likely mediated by a large infarct volume.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Clinical Relevance of Computed Tomography Perfusion-Estimated Infarct Volume in Acute Ischemic Stroke Patients within the 6-h Therapeutic Time Window.Cerebrovasc Dis. 2022;51(4):438-446. doi: 10.1159/000519901. Epub 2022 Jan 21. Cerebrovasc Dis. 2022. PMID: 35066495
-
Association of blood pressure and outcomes differs upon cerebral perfusion post-thrombectomy in patients with acute ischemic stroke.J Neurointerv Surg. 2024 May 2;17(5):500-507. doi: 10.1136/jnis-2024-021487. J Neurointerv Surg. 2024. PMID: 38697808
-
Hyperperfusion after Endovascular Reperfusion Therapy for Acute Ischemic Stroke.J Stroke Cerebrovasc Dis. 2019 May;28(5):1212-1218. doi: 10.1016/j.jstrokecerebrovasdis.2019.01.007. Epub 2019 Jan 28. J Stroke Cerebrovasc Dis. 2019. PMID: 30704865
-
Association of inflammatory and platelet volume markers with clinical outcome in patients with anterior circulation ischaemic stroke after endovascular thrombectomy.Neurol Res. 2021 Jun;43(6):503-510. doi: 10.1080/01616412.2020.1870359. Epub 2021 Jan 5. Neurol Res. 2021. PMID: 33402058
-
Plasma Lipid Mediators Associate With Clinical Outcome After Successful Endovascular Thrombectomy in Patients With Acute Ischemic Stroke.Front Immunol. 2022 Jul 4;13:917974. doi: 10.3389/fimmu.2022.917974. eCollection 2022. Front Immunol. 2022. PMID: 35865524 Free PMC article.
Cited by
-
Hyperemia detection on arterial spin labeling is associated with final infarct volume in stroke post-endovascular therapy.J Stroke Cerebrovasc Dis. 2025 Aug;34(8):108358. doi: 10.1016/j.jstrokecerebrovasdis.2025.108358. Epub 2025 May 26. J Stroke Cerebrovasc Dis. 2025. PMID: 40436255
References
-
- Fujimura M, et al. Efficacy of prophylactic blood pressure lowering according to a standardized postoperative management protocol to prevent symptomatic cerebral hyperperfusion after direct revascularization surgery for Moyamoya disease. Cerebrovasc. Dis. 2012;33:436–445. doi: 10.1159/000336765. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
