

Prevalence of metabolic syndrome among patients with hepatocellular carcinoma of different etiologies: a retrospective study
- PMID: 38693556
- PMCID: PMC11064370
- DOI: 10.1186/s13027-024-00575-6
Prevalence of metabolic syndrome among patients with hepatocellular carcinoma of different etiologies: a retrospective study
Abstract
Aims: This study compared the prevalences of metabolic syndrome and of cardiac or kidney comorbidities among patients with hepatocellular carcinoma (HCC) associated with metabolic dysfunction-related fatty liver disease (MAFLD), chronic infection with hepatitis B or C virus (HBV or HCV), or the combination of MAFLD and chronic HBV infection.
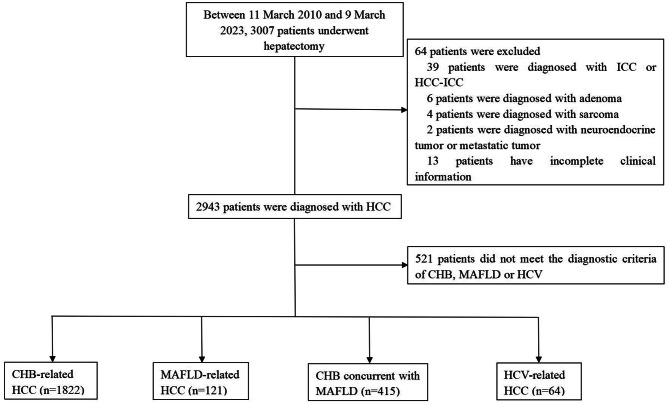
Methods: Medical records were retrospectively analyzed for patients with HCC who underwent hepatectomy between March 2013 and March 2023. Patients with HCC of different etiologies were compared in terms of their clinicodemographic characteristics and laboratory data before surgery.
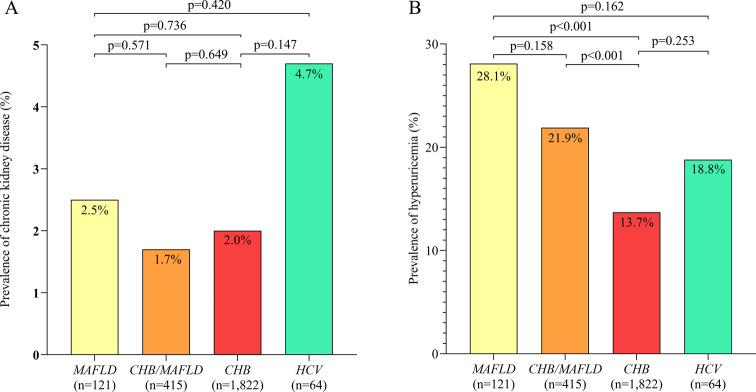
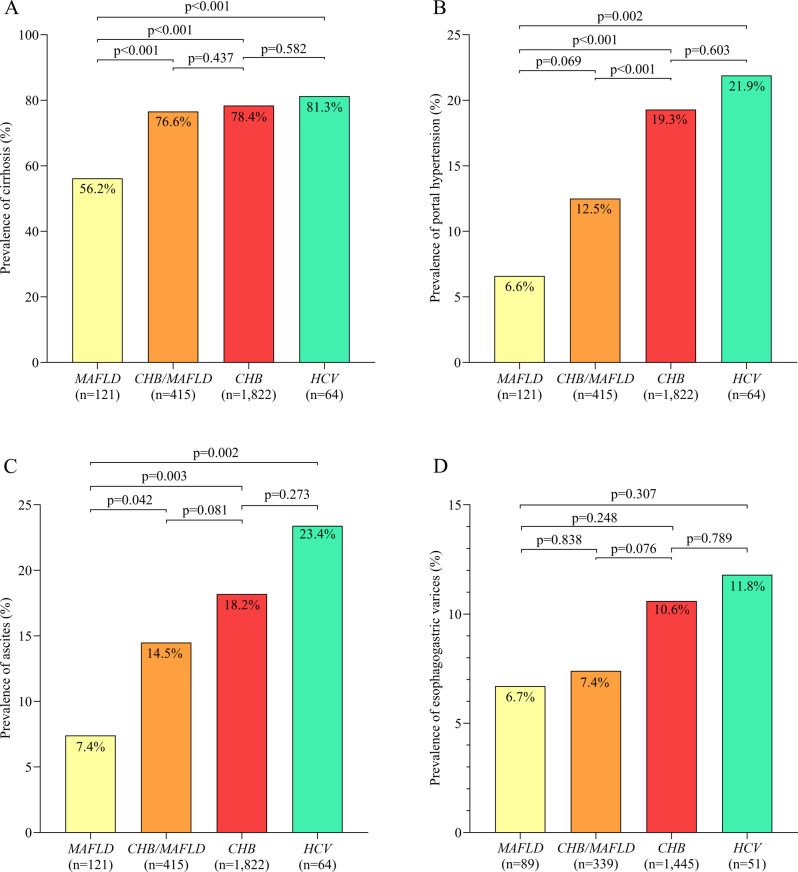
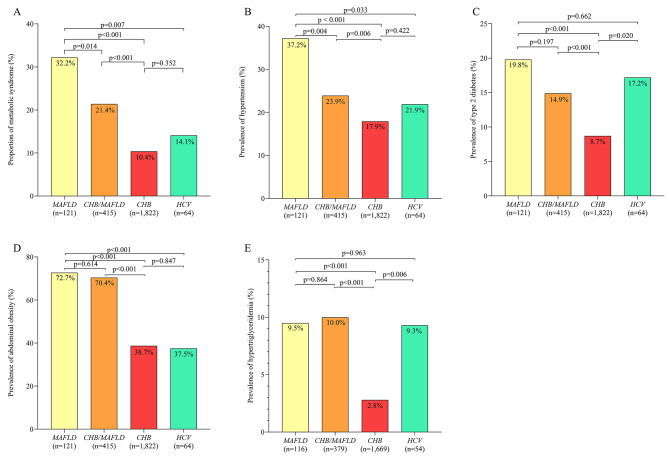
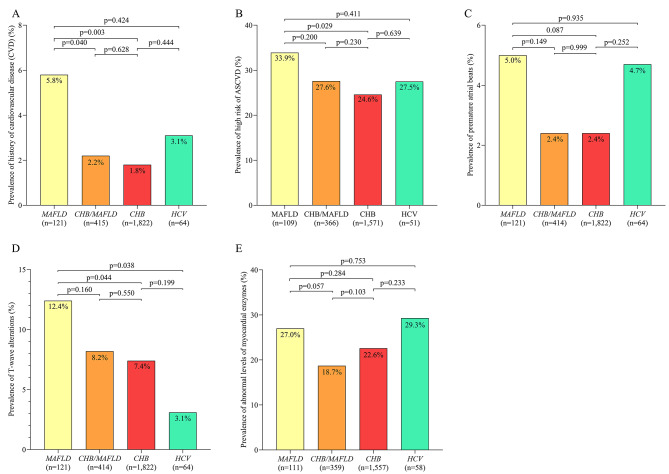
Results: Of the 2422 patients, 1,822 (75.2%) were chronically infected with HBV without MAFLD and HCV, 415 (17.2%) had concurrent MAFLD and chronic HBV infection but no HCV infection, 121 (5.0%) had MAFLD without hepatitis virus infection, and 64 (2.6%) were chronically infected with HCV in the presence or absence of MAFLD and HBV infection. Compared to patients chronically infected with HBV without MAFLD and HCV, those with MAFLD but no hepatitis virus infection showed significantly lower prevalence of cirrhosis, ascites, portal hypertension, alpha-fetoprotein concentration ≥ 400 ng/mL, tumor size > 5 cm, multinodular tumors and microvascular invasion. Conversely, they showed significantly higher prevalence of metabolic syndrome, hypertension, type 2 diabetes, abdominal obesity, history of cardiovascular disease, T-wave alterations, hypertriglyceridemia and hyperuricemia, as well as higher risk of arteriosclerotic cardiovascular disease. Compared to patients with MAFLD but no hepatitis virus infection, those with concurrent MAFLD and chronic infection with HBV showed significantly higher prevalence of cirrhosis, ascites and portal hypertension, but significantly lower prevalence of hypertension and history of cardiovascular disease. Compared to patients with other etiologies, those chronically infected with HCV in the presence or absence of MAFLD and HBV infection, showed significantly higher prevalence of cirrhosis, portal hypertension, ascites, and esophagogastric varices.
Conclusion: Patients with HCC associated with MAFLD tend to have a background of less severe liver disease than those with HCC of other etiologies, but they may be more likely to suffer metabolic syndrome or comorbidities affecting the heart or kidneys.
Keywords: Chronic hepatitis B; Hepatocellular carcinoma; Metabolic dysfunction-related fatty liver disease; Metabolic syndrome.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Hepatectomy for Metabolic Associated Fatty Liver Disease (MAFLD) related HCC: Propensity case-matched analysis with viral- and alcohol-related HCC.Eur J Surg Oncol. 2022 Jan;48(1):103-112. doi: 10.1016/j.ejso.2021.07.015. Epub 2021 Jul 24. Eur J Surg Oncol. 2022. PMID: 34325939
-
Impact of Metabolic Dysfunction-Associated Fatty Liver Disease on the Prognosis of Patients With Hepatocellular Carcinoma After Radical Resection: A Retrospective Study.Cureus. 2024 Dec 7;16(12):e75302. doi: 10.7759/cureus.75302. eCollection 2024 Dec. Cureus. 2024. PMID: 39781154 Free PMC article.
-
Impact of MAFLD on the complications after hepatectomy in patients with HBV-related hepatocellular carcinoma.Medicine (Baltimore). 2023 Mar 3;102(9):e33062. doi: 10.1097/MD.0000000000033062. Medicine (Baltimore). 2023. PMID: 36862923 Free PMC article.
-
Global prevalence of metabolic dysfunction-associated fatty liver disease-related hepatocellular carcinoma: A systematic review and meta-analysis.Clin Mol Hepatol. 2024 Jul;30(3):436-448. doi: 10.3350/cmh.2024.0109. Epub 2024 Apr 16. Clin Mol Hepatol. 2024. PMID: 38623613 Free PMC article.
-
Hepatitis C virus infection in black patients with hepatocellular carcinoma in southern Africa.Princess Takamatsu Symp. 1995;25:33-40. Princess Takamatsu Symp. 1995. PMID: 8875607 Review.
Cited by
-
The impact of metabolic syndrome on hepatocellular carcinoma: a mendelian randomization study.Sci Rep. 2025 Jan 14;15(1):1941. doi: 10.1038/s41598-025-86317-z. Sci Rep. 2025. PMID: 39809981 Free PMC article.
-
Systematic treatment in unresectable hepatocellular carcinoma: The most concerns.ILIVER. 2024 Aug 13;3(3):100112. doi: 10.1016/j.iliver.2024.100112. eCollection 2024 Sep. ILIVER. 2024. PMID: 40636090 Free PMC article. No abstract available.
References
-
- Akinyemiju T, Abera S, Ahmed M, Alam N, Alemayohu MA, Allen C, et al. The Burden of Primary Liver Cancer and underlying etiologies from 1990 to 2015 at the Global, Regional, and National Level: results from the global burden of Disease Study 2015. JAMA Oncol. 2017;3(12):1683–91. doi: 10.1001/jamaoncol.2017.3055. - DOI - PMC - PubMed
-
- Quek J, Chan KE, Wong ZY, Tan C, Tan B, Lim WH, et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2023;8(1):20–30. doi: 10.1016/S2468-1253(22)00317-X. - DOI - PubMed
Grants and funding
- 2300008/the Science and Technology Key Project of Guigang City
- GuiKe AD22035057/the Specific Research Project of Guangxi for Research Bases and Talents
- 82060510/he National Natural Science Foundation of China
- 82260569/the National Natural Science Foundation of China
- GKE-ZZ202217 and GKE-ZZ202311/the Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor (Guangxi Medical University), Ministry of Education
LinkOut - more resources
Full Text Sources
