

Chronic ACLD Knees with Early Developmental Cartilage Lesions Exhibited Increased Posterior Tibial Translation during Level Walking
- PMID: 38693612
- PMCID: PMC11144518
- DOI: 10.1111/os.14072
Chronic ACLD Knees with Early Developmental Cartilage Lesions Exhibited Increased Posterior Tibial Translation during Level Walking
Abstract
Objective: Early articular cartilage lesion (CL) is a vital sign in the onset of posttraumatic knee osteoarthritis (PTOA) in patients with anterior cruciate ligament deficiency (ACLD). Researchers have suggested that altered kinematics could accelerate CLs and, therefore, lead to the onset of PTOA. However, little is known about whether specific knee kinematics exist that lead to early CL in chronic ACLD knees. Level walking is the most frequent and relevant in vivo activity, which greatly impacts knee health. We hypothesized that the knee kinematics during level walking in chronic ACLD knees with early tibiofemoral CL would significantly differ from those of chronic ACLD knees without early tibiofemoral CL.
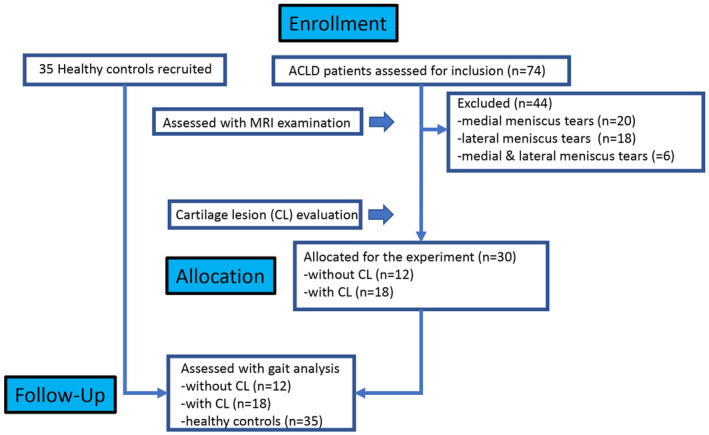
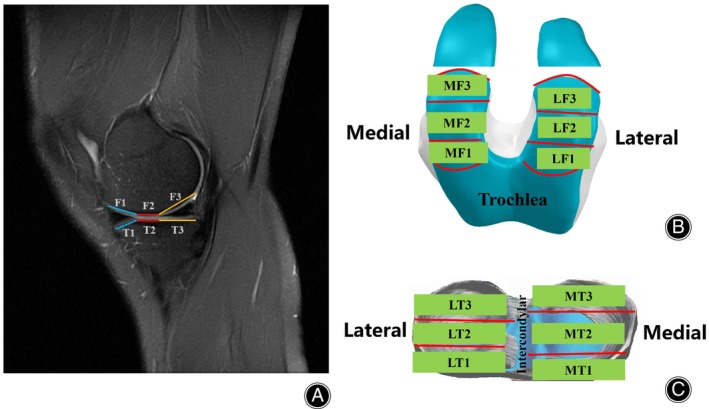
Methods: Thirty patients with a chronic ACLD history, including 18 subjects with CLs and 12 subjects without CLs, and 35 healthy control subjects were recruited for the study from July 2020 to August 2022. The knee kinematic data during level walking were collected using a three-dimensional motion analysis system. The kinematic differences between groups were compared using statistical parametric mapping with one dimension for One-Way ANOVA. The cartilage statuses of the ACLD knees were assessed via MRI examination. The CLs distribution of subjects was evaluated using a modified Noyes scale and analyzed by chi-square tests.
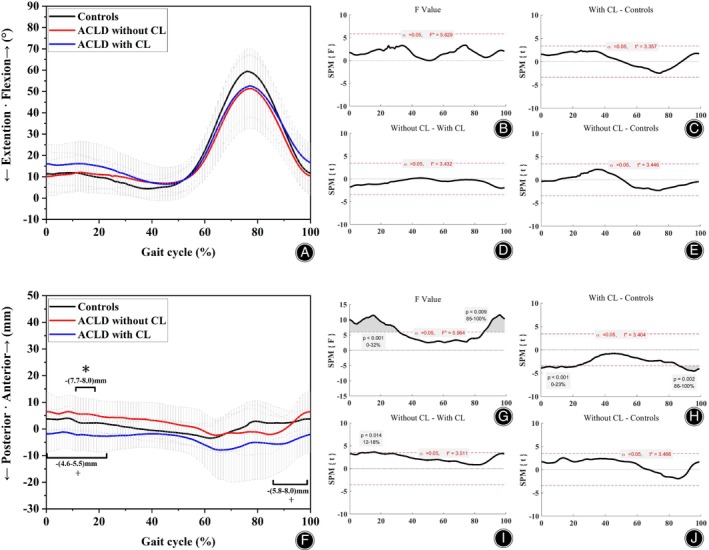
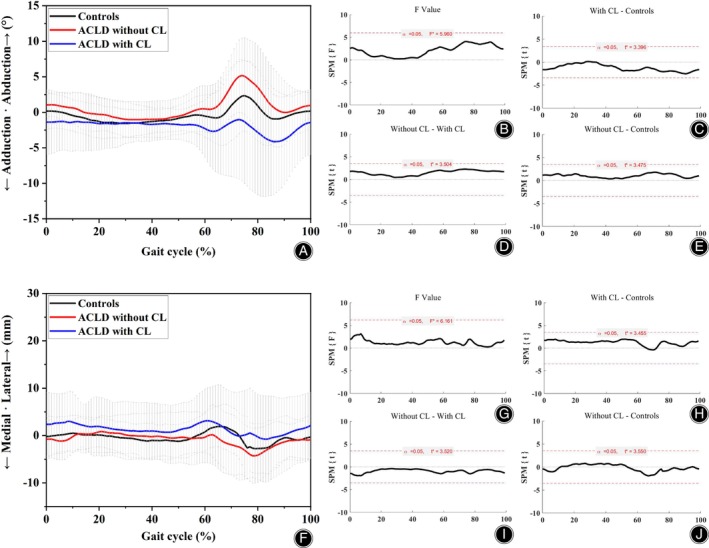
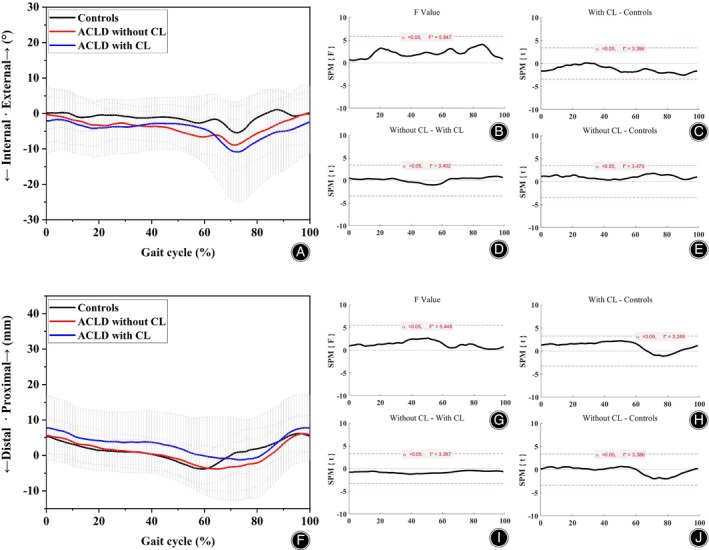
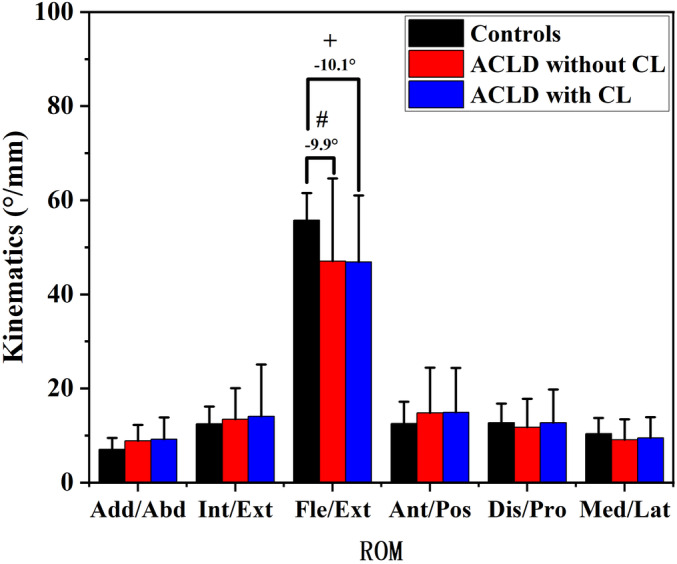
Results: ACLD knees with CLs had significantly greater posterior tibial translation (7.7-8.0mm, 12%-18% gait cycle GC, p = 0.014) compared to ACLD knees without CLs during level walking. ACLD knees with CLs had greater posterior tibial translation (4.6-5.5mm, 0%-23% GC, p < 0.001; 5.8-8.0mm, 86%-100% GC, p < 0.001) than healthy controls during level walking. In the group of ACLD knees with CLs, CL is mainly located in the back of the tibia plateau and front of load bearing area of the medial femoral condyle (p < 0.05).
Conclusion: Chronic anterior cruciate ligament deficient knees with cartilage lesions have increased posterior tibial translation compared to anterior cruciate ligament deficient knees without cartilage lesions and healthy subjects. The posterior tibial translation may play an important role in knee cartilage degeneration in ACLD knees. The increased posterior tibial translation and cartilage lesion characteristics may improve our understanding of the role of knee kinematics in cartilage degeneration and could be a helpful potential reference for anterior cruciate ligament deficient therapy, such as physical training to improve abnormal kinematic behavior.
Keywords: Anterior Cruciate Ligament Deficiency; Cartilage Lesion; Knee Kinematics; Level Walking; Post‐Traumatic Knee Osteoarthritis.
© 2024 The Authors. Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Figures
References
-
- Ajuied A, Wong F, Smith C, Norris M, Earnshaw P, Back D, et al. Anterior cruciate ligament injury and radiologic progression of knee osteoarthritis: a systematic review and meta‐analysis. Am J Sports Med. 2014;42(9):2242–2252. https://www.ncbi.nlm.nih.gov/pubmed/24214929 - PubMed
-
- Poulsen E, Goncalves GH, Bricca A, Roos EM, Thorlund JB, Juhl CB. Knee osteoarthritis risk is increased 4‐6 fold after knee injury – a systematic review and meta‐analysis. Br J Sports Med. 2019;53(23):1454–1463. https://www.ncbi.nlm.nih.gov/pubmed/31072840 - PubMed
-
- Bodkin SG, Werner BC, Slater LV, Hart JM. Post‐traumatic osteoarthritis diagnosed within 5 years following ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2020;28(3):790–796. https://www.ncbi.nlm.nih.gov/pubmed/30887068 - PubMed
-
- Glyn‐Jones S, Palmer AJ, Agricola R, Price AJ, Vincent TL, Weinans H, et al. Osteoarthritis. Lancet. 2015;386(9991):376–387. https://www.ncbi.nlm.nih.gov/pubmed/25748615 - PubMed
-
- Chaudhari AM, Briant PL, Bevill SL, Koo S, Andriacchi TP. Knee kinematics, cartilage morphology, and osteoarthritis after ACL injury. Med Sci Sports Exerc. 2008;40(2):215–222. https://www.ncbi.nlm.nih.gov/pubmed/18202582 - PubMed
MeSH terms
Grants and funding
- 2023B1212060063/Science and Technology Planning Project of Guangdong Province
- E43715/Shi Yangshan Academic Experience Inheritance Studio Construction Project
- E43607/Lingnan Orthopaedic School Inheritance Studio Construction Project
- 0103030912/Lin Dingkun's Guangdong Province Famous Traditional Chinese Medicine Inheritance Studio Construction Project
- Z155080000004/Project of Administration of Traditional Chinese Medicine of Guangdong Province
LinkOut - more resources
Full Text Sources
Miscellaneous
