

Definition and management of arrhythmia-induced cardiomyopathy: findings from the European Heart Rhythm Association survey
- PMID: 38693772
- PMCID: PMC11094751
- DOI: 10.1093/europace/euae112
Definition and management of arrhythmia-induced cardiomyopathy: findings from the European Heart Rhythm Association survey
Abstract
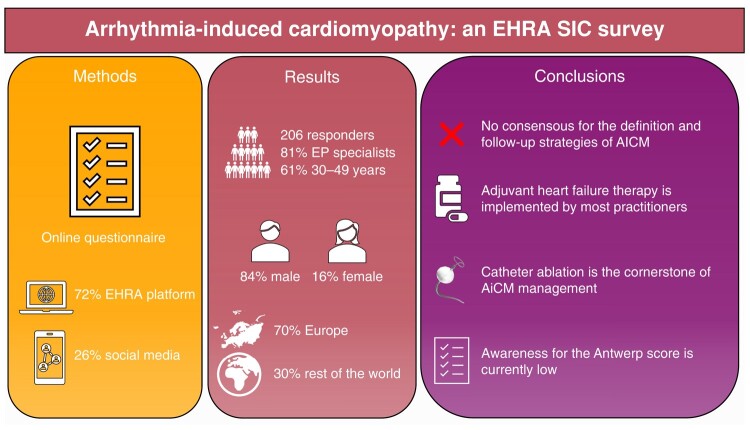
Aims: Arrhythmia-induced cardiomyopathy (AiCM) represents a subtype of acute heart failure (HF) in the context of sustained arrhythmia. Clear definitions and management recommendations for AiCM are lacking. The European Heart Rhythm Association Scientific Initiatives Committee (EHRA SIC) conducted a survey to explore the current definitions and management of patients with AiCM among European and non-European electrophysiologists.
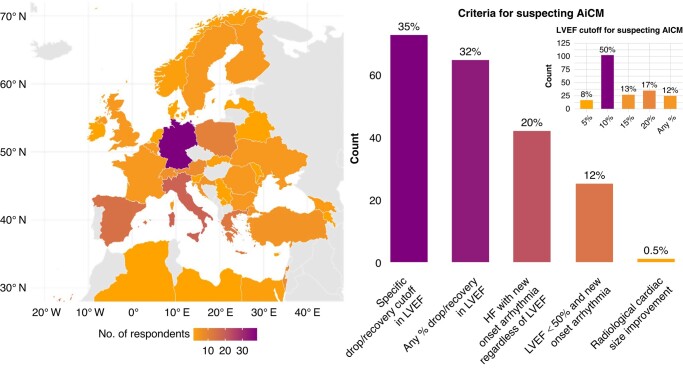
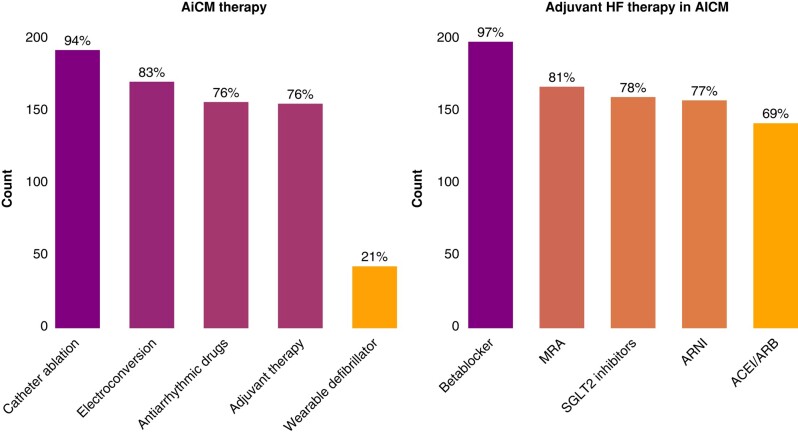
Methods and results: A 25-item online questionnaire was developed and distributed among EP specialists on the EHRA SIC website and on social media between 4 September and 5 October 2023. Of the 206 respondents, 16% were female and 61% were between 30 and 49 years old. Most of the respondents were EP specialists (81%) working at university hospitals (47%). While most participants (67%) agreed that AiCM should be defined as a left ventricular ejection fraction (LVEF) impairment after new onset of an arrhythmia, only 35% identified a specific LVEF drop to diagnose AiCM with a wide range of values (5-20% LVEF drop). Most respondents considered all available therapies: catheter ablation (93%), electrical cardioversion (83%), antiarrhythmic drugs (76%), and adjuvant HF treatment (76%). A total of 83% of respondents indicated that adjuvant HF treatment should be started at first HF diagnosis prior to antiarrhythmic treatment, and 84% agreed it should be stopped within six months after LVEF normalization. Responses for the optimal time point for the first LVEF reassessment during follow-up varied markedly (1 day-6 months after antiarrhythmic treatment).
Conclusion: This EHRA Survey reveals varying practices regarding AiCM among physicians, highlighting a lack of consensus and heterogenous care of these patients.
Keywords: Antwerp score; Arrhythmia-induced cardiomyopathy; Atrial fibrillation; Heart failure; Pacemaker; Premature ventricular contractions.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: T.S. has received research funding from the Swiss Academy of Medical Sciences and the ‘Gottfried & Julia Bangerter-Rhyner’ Foundation. P.B. has received research funding from the ‘University of Basel’, the ‘Stiftung für Herzschrittmacher und Elektrophysiologie’, the ‘Freiwillige Akademische Gesellschaft Basel’, and Johnson&Johnson, all outside the submitted work and reports personal fees from Abbott. M.K. reports grants from Bayer, grants from BMS, grants from Boston Scientific, grants from Daiichi Sankyo, grants from Pfizer, personal fees from Abbott, personal fees from Boston Scientific, and personal fees from Daiichi Sankyo, all outside the submitted work. C.S. is a Member of Medtronic Advisory Board Europe and Boston Scientific Advisory Board Europe, received educational grants from Biosense Webster and Biotronik and a research grant from the European Union’s FP7 programme and Biosense Webster, and lecture and consulting fees from Abbott, Medtronic, Biosense-Webster, Boston Scientific, Microport, and Biotronik, all outside the submitted work J.d.F.d.L. has received research funding from the ‘University of Basel’ and from the ‘Swiss Heart Foundation’. The remaining authors have nothing to declare. The production of this document is under the responsibility of the Scientific Initiatives Committee of the European Heart Rhythm Association: Julian K.R. Chun (Chair), Sergio Castrejon (Co-Chair), Ante Anic, Giulio Conte, Piotr Futyma, Andreas Metzner, Federico Migliore, Giacomo Mugnai, Laura Perrotta, Rui Providencia, Sergio Richter, Laurent Roten, and Arian Sultan. The authors acknowledge the EHRA Scientific Research Network centres participating in this survey. A list of these centres can be found on the EHRA website.
Figures
References
-
- Simantirakis EN, Koutalas EP, Vardas PE. Arrhythmia-induced cardiomyopathies: the riddle of the chicken and the egg still unanswered? Europace 2012;14:466–73. - PubMed
-
- Hékimian G, Paulo N, Waintraub X, Bréchot N, Schmidt M, Lebreton G et al. Arrhythmia-induced cardiomyopathy: a potentially reversible cause of refractory cardiogenic shock requiring venoarterial extracorporeal membrane oxygenation. Heart Rhythm 2021;18:1106–12. - PubMed
-
- Raymond-Paquin A, Nattel S, Wakili R, Tadros R. Mechanisms and clinical significance of arrhythmia-induced cardiomyopathy. Canad J Cardiol 2018;34:1449–60. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
