

Arthroscopic suture bridge fixation for acute bony Bankart with anterior glenohumeral instability: a case report and narrative review
- PMID: 38694813
- PMCID: PMC11061656
- DOI: 10.21037/aoj-23-46
Arthroscopic suture bridge fixation for acute bony Bankart with anterior glenohumeral instability: a case report and narrative review
Abstract
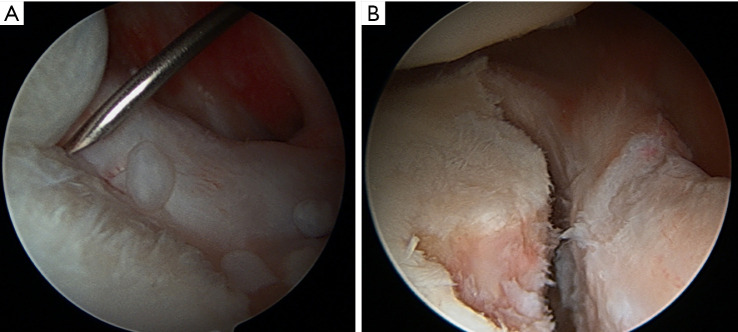
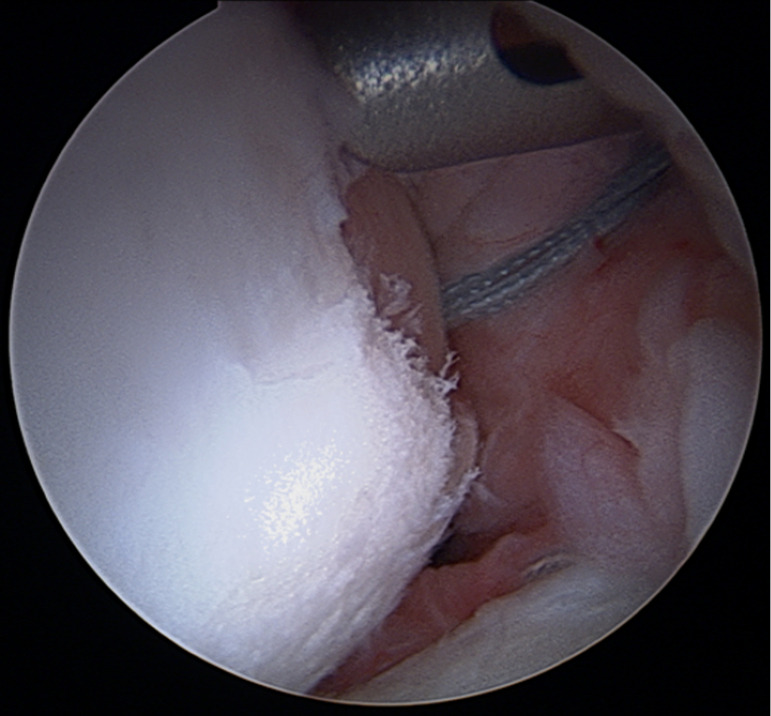
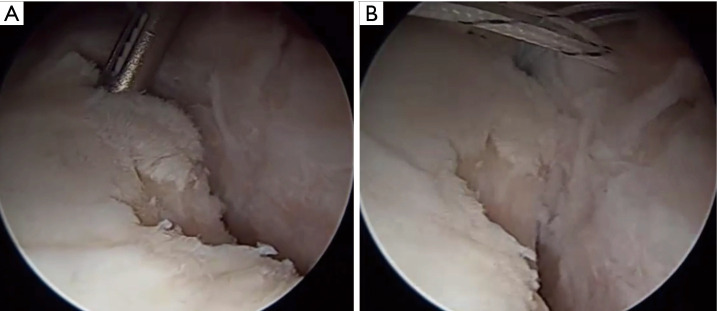
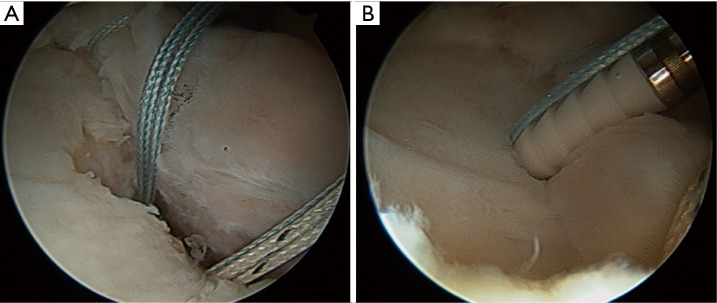
Background and objective: Anterior shoulder dislocations can result in acute glenoid rim fractures that compromise the bony stability of the glenohumeral joint. Adequate fixation of these fractures is required to restore stability, decrease shoulder pain, and facilitate return to activity. The double-row suture bridge is a relatively novel fixation technique, first described in 2009, that accomplishes internal fixation with sufficient stability using an all-arthroscopic technique to restore the glenoid footprint. A 40-year-old female with recurrent anterior shoulder instability in the setting of seizure disorder was found to have a bony Bankart lesion of 25% to 30% with a concomitant superior labral tear. The patient was treated with a double-row bony Bankart bridge and labral repair. At six months follow-up, she has progressed to a full recovery with no recurrence.
Methods: A search was conducted in May 2023 in PubMed, EMBASE, and CINAHL with the search terms bony Bankart, bone Bankart, osseous Bankart, acute, bridge, suture bridge, double row.
Key content and findings: Double-row suture bridge repairs result in improvement in shoulder function as determined by ASES (93.5), QuickDASH (4.5), SANE (95.9), and SF-12 (55.6). The overall recurrence rate of anterior instability after a bony Bankart bridge repair is 8%. When examining the return to prior level of function, 81.4% of patients were able to do so with only 7.9% of patients reporting significant modifications to their activity level. In mid-term results, double row suture bridge demonstrates similar outcomes to other all-arthroscopic fixation methods of bony Bankart injuries. Importantly, bony Bankart bridge remains a viable option for critical glenoid lesions over the 20% cutoff used in other all arthroscopic techniques. Biomechanically, the double-row suture bridge offers distinct benefits over its single-row counterpart including increased compression, reduced displacement, and reduced step-off.
Conclusions: Although there is limited data, the studies discussed and the demonstrative case show the potential benefit of all-arthroscopic double-row suture bridge fixation including increased compression, decreased displacement, and a lower complication rate in patients with large bony Bankart lesions traditionally requiring bony augmentation. However, more robust studies are necessary to determine the long-term success of the double-row suture bridge.
Keywords: Glenoid bone loss; bony Bankart; double-row; shoulder arthroscopy; suture bridge.
2024 Annals of Joint. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://aoj.amegroups.com/article/view/10.21037/aoj-23-46/coif). The series “Bone Loss in Shoulder Instability and Shoulder Arthroplasty” was commissioned by the editorial office without any funding or sponsorship. N.A.T. declares that he is a paid presenter or speaker of DJ Orthopaedics. B.R.W. declares that he receives publishing royalties from Arthroscopy and Elsevier, works as a paid consultant for DePuy and FH Ortho, works as a paid presenter for Arthrex and Vericel, serves on the board member of American Academy of Orthopaedic Surgeons, Arthroscopy, American Orthopaedic Society for Sports Medicine, American Association of Nurse Anesthesiology and American Shoulder and Elbow Society, and serves on the editorial or governing board of The Video Journal of Sports Medicine. He also holds stock or stock options of Kaliber AI, Sparta and Vivorte, and has other financial or material support from Musculosckelatal transplant foundation and Smith and Nephew. The authors have no other conflicts of interest to declare.
Figures










Similar articles
-
Arthroscopic Double-Row Suture Anchor Repair of Acute Posterior Bony Bankart Lesion.Arthrosc Tech. 2016 Aug 8;5(4):e839-e843. doi: 10.1016/j.eats.2016.04.004. eCollection 2016 Aug. Arthrosc Tech. 2016. PMID: 27709046 Free PMC article.
-
A Biomechanical, Cadaveric Evaluation of Single- Versus Double-Row Repair Techniques on Stability of Bony Bankart Lesions.Am J Sports Med. 2021 Mar;49(3):773-779. doi: 10.1177/0363546520985184. Epub 2021 Feb 5. Am J Sports Med. 2021. PMID: 33544626
-
Suture anchor fixation of bony Bankart fractures: comparison of single-point with double-point "suture bridge" technique.Am J Sports Med. 2013 Nov;41(11):2624-31. doi: 10.1177/0363546513501795. Epub 2013 Sep 5. Am J Sports Med. 2013. PMID: 24007759
-
Clinical Outcomes of Arthroscopic Bony Bankart Repair for Anterior Instability of the Shoulder: A Systematic Review.Am J Sports Med. 2023 Aug;51(10):2758-2765. doi: 10.1177/03635465221094832. Epub 2022 Jun 24. Am J Sports Med. 2023. PMID: 35749344
-
Arthroscopic Bankart Repair With Remplissage in Comparison to Bone Block Augmentation for Anterior Shoulder Instability With Bipolar Bone Loss: A Systematic Review.Arthroscopy. 2021 Feb;37(2):706-717. doi: 10.1016/j.arthro.2020.08.033. Epub 2020 Sep 7. Arthroscopy. 2021. PMID: 32911004
Cited by
-
Arthroscopic Bankart Repair Using 1 Anterior Portal Has a Shorter Surgical Time and Comparable Clinical Results With the Standard 2-Portal Technique.Arthrosc Sports Med Rehabil. 2024 Jul 26;6(6):100984. doi: 10.1016/j.asmr.2024.100984. eCollection 2024 Dec. Arthrosc Sports Med Rehabil. 2024. PMID: 39776508 Free PMC article.
References
-
- Midtgaard KS, Bøe B, Lundgreen K, et al. Anterior shoulder dislocation - assessment and treatment. Tidsskr Nor Laegeforen 2021. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical