

Associations Between Volume of Early Intravenous Fluid and Hospital Outcomes in Septic Patients With and Without Heart Failure: A Retrospective Cohort Study
- PMID: 38694845
- PMCID: PMC11057813
- DOI: 10.1097/CCE.0000000000001082
Associations Between Volume of Early Intravenous Fluid and Hospital Outcomes in Septic Patients With and Without Heart Failure: A Retrospective Cohort Study
Abstract
Objectives: To evaluate the relationship between early IV fluid volume and hospital outcomes, including death in-hospital or discharge to hospice, in septic patients with and without heart failure (HF).
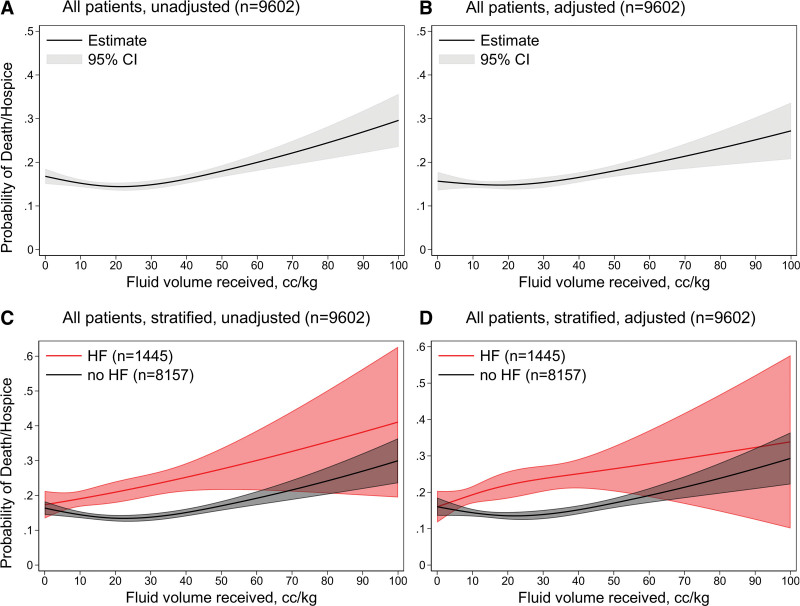
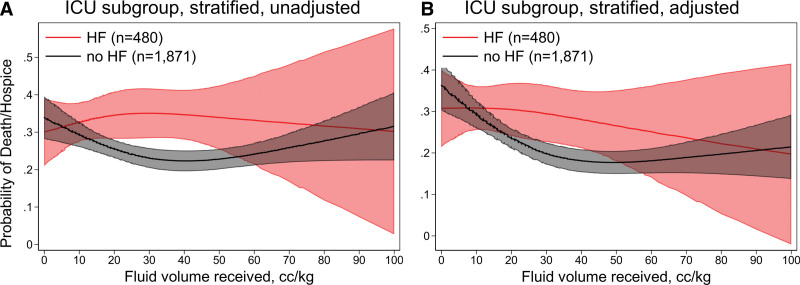
Design: A retrospective cohort study using logistic regression with restricted cubic splines to assess for nonlinear relationships between fluid volume and outcomes, stratified by HF status and adjusted for propensity to receive a given fluid volume in the first 6 hours. An ICU subgroup analysis was performed. Secondary outcomes of vasopressor use, mechanical ventilation, and length of stay in survivors were assessed.
Setting: An urban university-based hospital.
Patients: A total of 9613 adult patients were admitted from the emergency department from 2012 to 2021 that met electronic health record-based Sepsis-3 criteria. Preexisting HF diagnosis was identified by the International Classification of Diseases codes.
Interventions: None.
Measurements and main results: There were 1449 admissions from patients with HF. The relationship between fluid volume and death or discharge to hospice was nonlinear in patients without HF, and approximately linear in patients with HF. Receiving 0-15 mL/kg in the first 6 hours was associated with lower likelihood of death or discharge to hospice compared with 30-45 mL/kg (odds ratio = 0.61; 95% CI, 0.41-0.90; p = 0.01) in HF patients, but no significant difference for non-HF patients. A similar pattern was identified in ICU admissions and some secondary outcomes. Volumes larger than 15-30 mL/kg for non-HF patients and 30-45 mL/kg for ICU-admitted non-HF patients were not associated with improved outcomes.
Conclusions: Early fluid resuscitation showed distinct patterns of potential harm and benefit between patients with and without HF who met Sepsis-3 criteria. Restricted cubic splines analysis highlighted the importance of considering nonlinear fluid outcomes relationships and identified potential points of diminishing returns (15-30 mL/kg across all patients without HF and 30-45 mL/kg when admitted to the ICU). Receiving less than 15 mL/kg was associated with better outcomes in HF patients, suggesting small volumes may be appropriate in select patients. Future studies may benefit from investigating nonlinear fluid-outcome associations and a focus on other conditions like HF.
Keywords: fluid therapy; heart failure; intensive care units; regression analysis; sepsis.
Copyright © 2024 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Figures

Similar articles
-
Fluid administration in severe sepsis and septic shock, patterns and outcomes: an analysis of a large national database.Intensive Care Med. 2017 May;43(5):625-632. doi: 10.1007/s00134-016-4675-y. Epub 2017 Jan 27. Intensive Care Med. 2017. PMID: 28130687
-
Optimal fluid resuscitation targets in septic patients with acutely decompensated heart failure.BMC Med. 2024 Oct 24;22(1):492. doi: 10.1186/s12916-024-03715-2. BMC Med. 2024. PMID: 39448976 Free PMC article.
-
Assessment of Outcomes in Patients with Heart Failure and End-Stage Kidney Disease after Fluid Resuscitation for Sepsis and Septic Shock.J Emerg Med. 2024 Jun;66(6):e670-e679. doi: 10.1016/j.jemermed.2024.02.001. Epub 2024 Feb 16. J Emerg Med. 2024. PMID: 38777707
-
Conservative versus liberal fluid resuscitation for septic patients at risk for fluid overload: A systematic review with meta-analysis.J Crit Care. 2025 Jun;87:155045. doi: 10.1016/j.jcrc.2025.155045. Epub 2025 Feb 28. J Crit Care. 2025. PMID: 40023080
-
Outcomes of CMS-mandated fluid administration among fluid-overloaded patients with sepsis: A systematic review and meta-analysis.Am J Emerg Med. 2022 May;55:157-166. doi: 10.1016/j.ajem.2022.03.004. Epub 2022 Mar 10. Am J Emerg Med. 2022. PMID: 35338881
Cited by
-
European Society of Intensive Care Medicine (ESICM) 2025 clinical practice guideline on fluid therapy in adult critically ill patients: part 2-the volume of resuscitation fluids.Intensive Care Med. 2025 Mar;51(3):461-477. doi: 10.1007/s00134-025-07840-1. Epub 2025 Mar 31. Intensive Care Med. 2025. PMID: 40163133
-
Unsupervised learning-derived phenotypes for personalized fluid management in critically ill patients with heart failure: A multicenter study.Clin Transl Med. 2024 Nov;14(11):e70081. doi: 10.1002/ctm2.70081. Clin Transl Med. 2024. PMID: 39514235 Free PMC article. No abstract available.
References
-
- Kaukonen K-M, Bailey M, Suzuki S, et al. : Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012. JAMA 2014; 311:1308–1316 - PubMed
-
- Liu V, Escobar GJ, Greene JD, et al. : Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA 2014; 312:90–92 - PubMed
-
- Kaukonen K-M, Bailey M, Pilcher D, et al. : Systemic inflammatory response syndrome criteria in defining severe sepsis. N Engl J Med 2015; 372:1629–1638 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
