

Meningioma: International Consortium on Meningiomas consensus review on scientific advances and treatment paradigms for clinicians, researchers, and patients
- PMID: 38695575
- PMCID: PMC11449035
- DOI: 10.1093/neuonc/noae082
Meningioma: International Consortium on Meningiomas consensus review on scientific advances and treatment paradigms for clinicians, researchers, and patients
Abstract
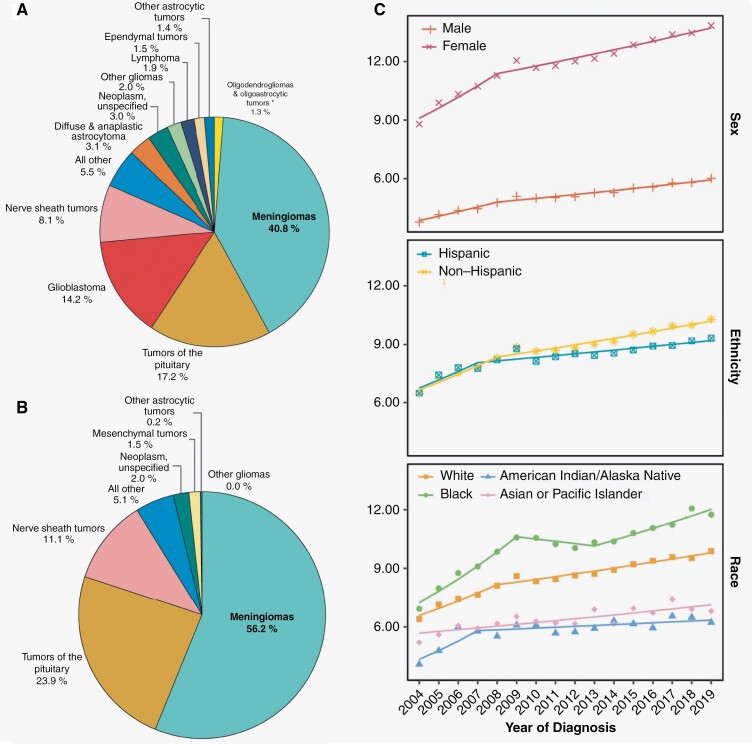
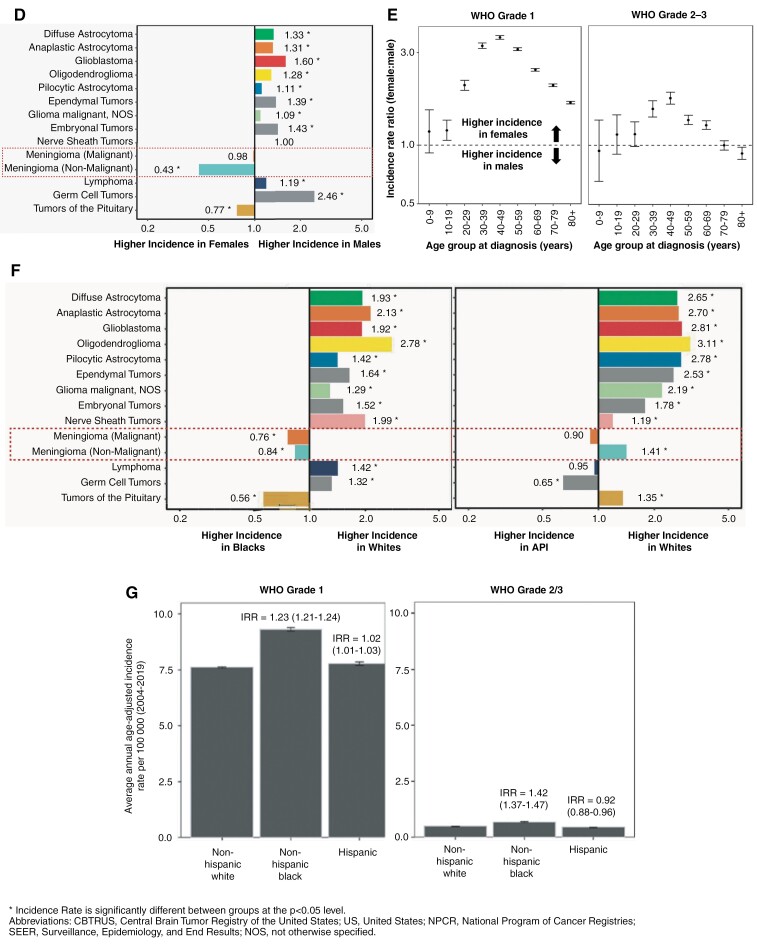
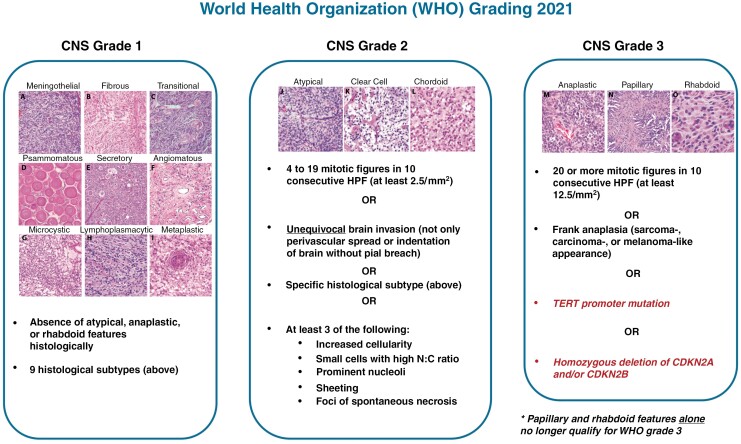
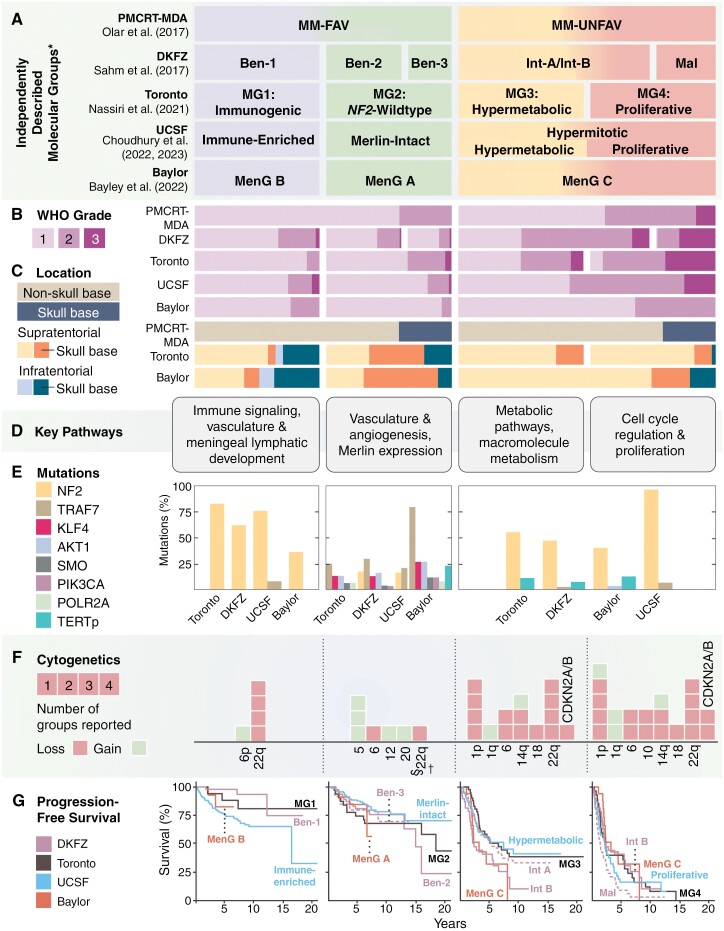
Meningiomas are the most common primary intracranial tumors in adults and are increasing in incidence due to the aging population and increased access to neuroimaging. While most exhibit nonmalignant behavior, a subset of meningiomas are biologically aggressive and are associated with treatment resistance, resulting in significant neurologic morbidity and even mortality. In recent years, meaningful advances in our understanding of the biology of these tumors have led to the incorporation of molecular biomarkers into their grading and prognostication. However, unlike other central nervous system (CNS) tumors, a unified molecular taxonomy for meningiomas has not yet been established and remains an overarching goal of the Consortium to Inform Molecular and Practical Approaches to CNS Tumor Taxonomy-Not Official World Health Organization (cIMPACT-NOW) working group. Additionally, clinical equipoise still remains on how specific meningioma cases and patient populations should be optimally managed. To address these existing gaps, members of the International Consortium on Meningiomas including field-leading experts, have prepared this comprehensive consensus narrative review directed toward clinicians, researchers, and patients. Included in this manuscript are detailed overviews of proposed molecular classifications, novel biomarkers, contemporary treatment strategies, trials on systemic therapies, health-related quality-of-life studies, and management strategies for unique meningioma patient populations. In each section, we discuss the current state of knowledge as well as ongoing clinical and research challenges to road map future directions for further investigation.
Keywords: extra-axial; meningioma; methylation; molecular; neurofibromatosis 2; nonmalignant; radiotherapy.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Figures
References
-
- Maier AD, Mirian C, Haslund-Vinding J, et al. Granular clinical history and outcome in 51 patients with primary and secondary malignant meningioma. J Neurosurg. 2022;137(5):1347–1357. - PubMed
-
- Tosefsky K, Rebchuk AD, Wang JZ, et al. Grade 3 meningioma survival and recurrence outcomes in an international multicenter cohort. J Neurosurg. 2023;140(2):393–403. - PubMed
