

Minimal Residual Disease using a Plasma-Only Circulating Tumor DNA Assay to Predict Recurrence of Metastatic Colorectal Cancer Following Curative Intent Treatment
- PMID: 38695832
- PMCID: PMC11247320
- DOI: 10.1158/1078-0432.CCR-23-3660
Minimal Residual Disease using a Plasma-Only Circulating Tumor DNA Assay to Predict Recurrence of Metastatic Colorectal Cancer Following Curative Intent Treatment
Abstract
Purpose: Minimal residual disease (MRD) detection can identify the recurrence in patients with colorectal cancer (CRC) following definitive treatment. We evaluated a plasma-only MRD assay to predict recurrence and survival in patients with metastatic CRC who underwent curative intent procedures (surgery and/or radiotherapy), with or without (neo)adjuvant chemotherapy. The primary objective of this study was to assess the correlation of postprocedure tumor cell-free DNA detection status with radiographic disease recurrence.
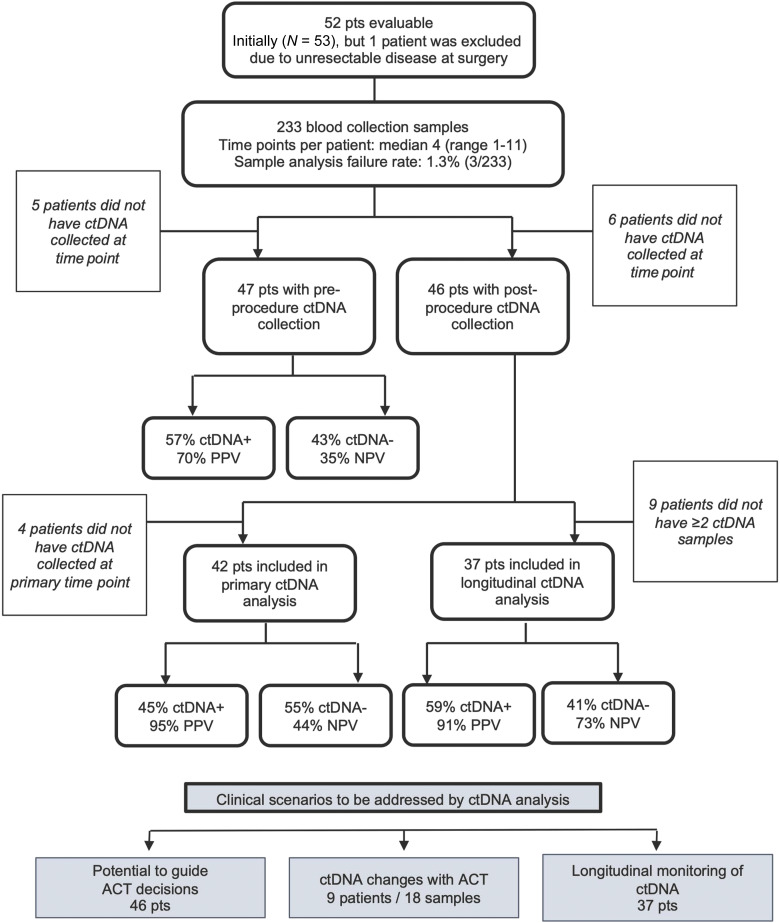
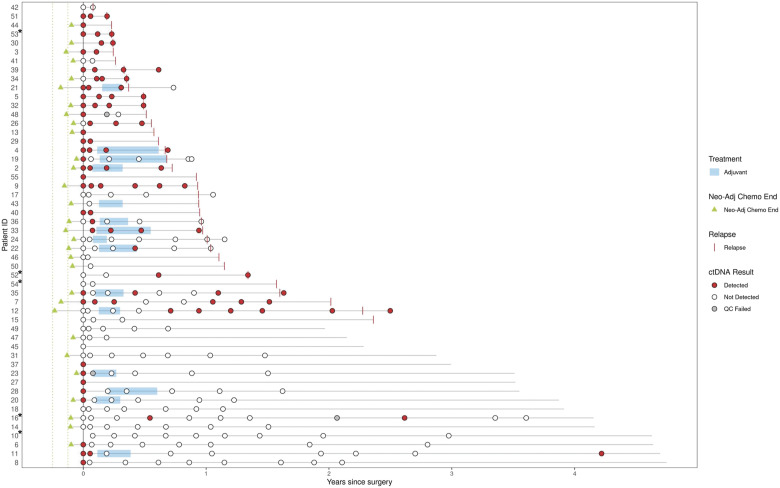
Experimental design: Preprocedure and postprocedure longitudinal samples were collected from 53 patients and analyzed with a multiomic MRD assay detecting circulating tumor DNA (ctDNA) from genomic and epigenomic signals. Preprocedure and postprocedure ctDNA detection correlated with recurrence-free and overall survival (OS).
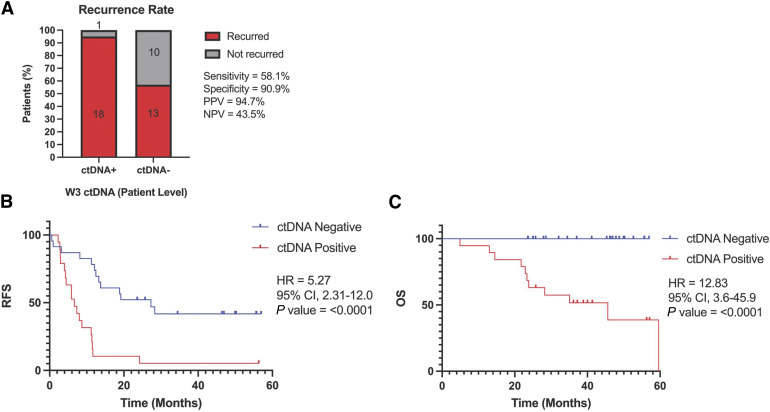
Results: From 52 patients, 230/233 samples were successfully analyzed. At the time of data cutoff, 36 (69.2%) patients recurred with median follow-up of 31 months. Detectable ctDNA was observed in 19/42 patients (45.2%) with ctDNA analyzed 3 weeks postprocedure. ctDNA detection 3 weeks postprocedure was associated with shorter median recurrence-free survival (RFS; HR, 5.27; 95% CI, 2.31-12.0; P < 0.0001) and OS (HR, 12.83; 95% CI, 3.6-45.9; P < 0.0001). Preprocedure ctDNA detection status was not associated with RFS but was associated with improved OS (HR, 4.65; 95% CI, 1.4-15.2; P = 0.0111). Undetectable ctDNA preprocedure had notable long-term OS, >90% 3 years postprocedure.
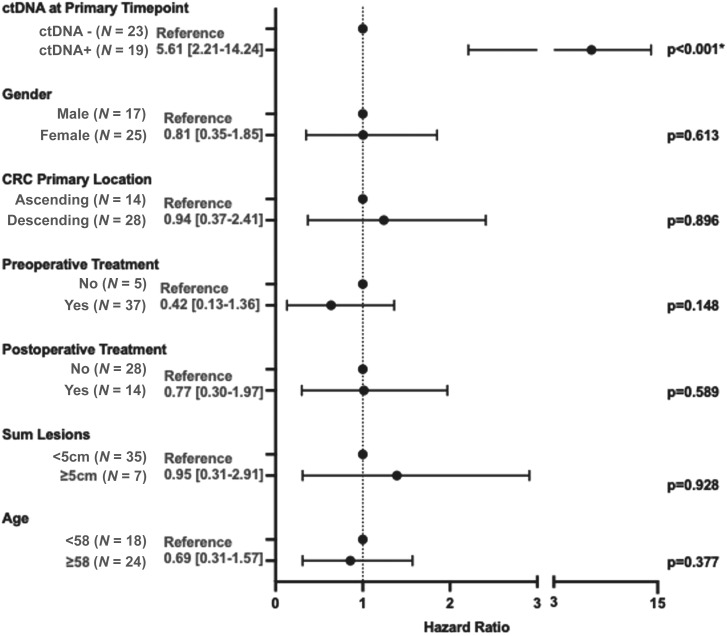
Conclusions: In this cohort of oligometastatic CRC, detection of ctDNA preprocedure or postprocedure was associated with inferior outcomes even after accounting for known prognostic clinicopathologic variables. This suggests ctDNA may enhance current risk stratification methods helping the evaluation of novel treatments and surveillance strategies toward improving patient outcomes.
©2024 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
A.R. Parikh reports grants from Guardant during the conduct of the study, as well as equity in C2i Genomics, XGenomes, Cadex, Vionix, and Parithera. A.R. Parikh also reports being an advisor/consultant for Eli Lilly, Mirati, Pfizer, Inivata, Biofidelity, Checkmate Pharmaceuticals, FMI, Guardant, AbbVie, Bayer, Delcath, Taiho, CVS, Value Analytics Lab, Seagen, Saga, AstraZeneca, Scare Inc., Illumina, Taiho, Hookipa, Kahar Medical, Xilio Therapeutics, Sirtex, Takeda, and Science For America; fees from UpToDate; travel fees from Karkinos Healthcare; being on the DSMC for a Roche study and on the Steering Committee for Exilixis; and research funding to institution from PureTech, PMV Pharmaceuticals, Plexxicon, Takeda, BMS, Mirati, Novartis, Erasca, Genentech, Daiichi Sankyo, Syndax, Revolution Medicine, and Parthenon. J. Tsai reports other support from Guardant Health outside the submitted work, and is a shareholder with Guardant Health. T.A. Rich reports employment and stock holdings of Guardant Health. K.S. Price reports other support from Guardant Health during the conduct of the study, as well as other support from Guardant Health outside the submitted work. L. Zhang reports personal fees from Samay Inc. and Smith-Kettlewell Eye Research Institute outside the submitted work. E.E. Van Seventer reports other support from Blueprint Medicines outside the submitted work. V.M. Raymond reports other support from Guardant Health during the conduct of the study, as well as other support from Guardant Health outside the submitted work. R.B. Corcoran reports personal fees from Guardant and Natera, as well as personal fees and other support from nRichDx, Alterome Therapeutics, and Sidewinder Therapeutics outside the submitted work. K. Van Loon reports other support from Natera outside the submitted work. C.E. Atreya reports other support from Guardant Health during the conduct of the study, as well as other support from Inivata, Roche/GNE, Pfizer, Novartis, Merck, Bristol-Myers Squibb, Erasca, and Gossamer Bio outside the submitted work. No disclosures were reported by the other authors.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004;350:2335–42. - PubMed
-
- Kawaguchi Y, Vauthey JN. The landmark series: randomized control trials examining perioperative chemotherapy and postoperative adjuvant chemotherapy for resectable colorectal liver metastasis. Ann Surg Oncol 2020;27:4263–70. - PubMed
