

The effectiveness of personalised surveillance and aftercare in breast cancer follow-up: a systematic review
- PMID: 38695938
- PMCID: PMC11065941
- DOI: 10.1007/s00520-024-08530-2
The effectiveness of personalised surveillance and aftercare in breast cancer follow-up: a systematic review
Abstract
Purpose: Breast cancer follow-up (surveillance and aftercare) varies from one-size-fits-all to more personalised approaches. A systematic review was performed to get insight in existing evidence on (cost-)effectiveness of personalised follow-up.
Methods: PubMed, Scopus and Cochrane were searched between 01-01-2010 and 10-10-2022 (review registered in PROSPERO:CRD42022375770). The inclusion population comprised nonmetastatic breast cancer patients ≥ 18 years, after completing curative treatment. All intervention-control studies studying personalised surveillance and/or aftercare designed for use during the entire follow-up period were included. All review processes including risk of bias assessment were performed by two reviewers. Characteristics of included studies were described.
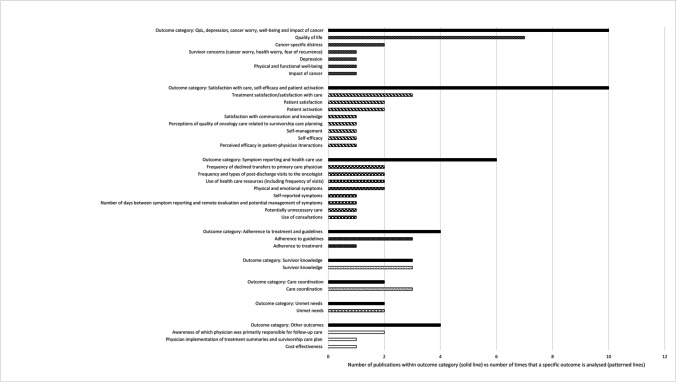
Results: Overall, 3708 publications were identified, 64 full-text publications were read and 16 were included for data extraction. One study evaluated personalised surveillance. Various personalised aftercare interventions and outcomes were studied. Most common elements included in personalised aftercare plans were treatment summaries (75%), follow-up guidelines (56%), lists of available supportive care resources (38%) and PROs (25%). Control conditions mostly comprised usual care. Four out of seven (57%) studies reported improvements in quality of life following personalisation. Six studies (38%) found no personalisation effect, for multiple outcomes assessed (e.g. distress, satisfaction). One (6.3%) study was judged as low, four (25%) as high risk of bias and 11 (68.8%) as with concerns.
Conclusion: The included studies varied in interventions, measurement instruments and outcomes, making it impossible to draw conclusions on the effectiveness of personalised follow-up. There is a need for a definition of both personalised surveillance and aftercare, whereafter outcomes can be measured according to uniform standards.
Keywords: Aftercare; Breast cancer; Personalised follow-up; Surveillance.
© 2024. The Author(s).
Conflict of interest statement
MvM, JK, MvH, ES, AZ, AK, CD and SS are involved in a large multicentre study evaluating (cost-)effectiveness of personalised surveillance and aftercare in the Netherlands (NABOR study, ZonMw project number 10330032010001).
Figures


References
-
- van der Meer DJ, Kramer I, van Maaren MC, van Diest PJ, S CL, Maduro JH, , et al. Comprehensive trends in incidence, treatment, survival and mortality of first primary invasive breast cancer stratified by age, stage and receptor subtype in the Netherlands between 1989 and 2017. Int J Cancer. 2021;148(9):2289–303. doi: 10.1002/ijc.33417. - DOI - PMC - PubMed
-
- West of Scotland Cancer Network. Breast Cancer Regional Follow-up Guideline v3.0. 2024. https://www.woscan.scot.nhs.uk/wp-content/uploads/Final-published_Breast.... Accessed on 15 Mar 2024
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
