

Penicillin Allergy Testing and Delabeling for Patients Who Are Prescribed Penicillin: A Systematic Review for a World Health Organization Guideline
- PMID: 38696031
- PMCID: PMC11193836
- DOI: 10.1007/s12016-024-08988-2
Penicillin Allergy Testing and Delabeling for Patients Who Are Prescribed Penicillin: A Systematic Review for a World Health Organization Guideline
Abstract
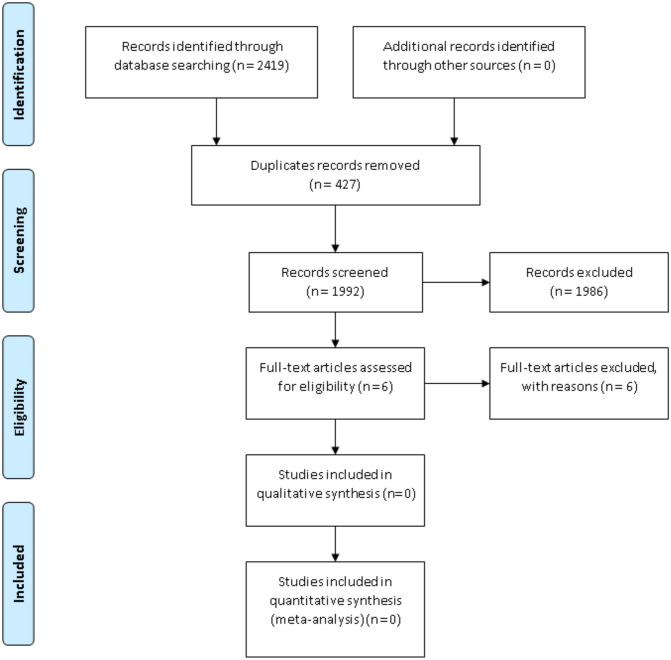
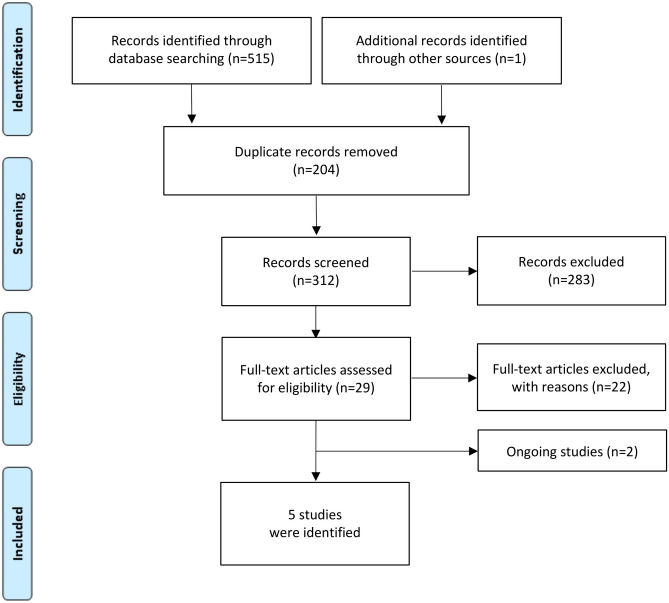
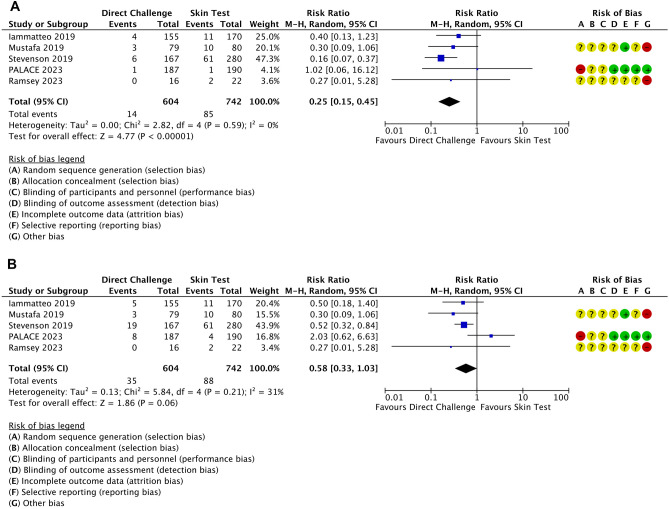
Secondary prevention with penicillin aims to prevent further episodes of acute rheumatic fever and subsequent development of rheumatic heart disease (RHD). Penicillin allergy, self-reported by 10% of the population, can affect secondary prevention programs. We aimed to assess the role for (i) routine penicillin allergy testing and the (ii) safety of penicillin allergy delabeling approaches in this context. We searched MEDLINE, Embase, CENTRAL, ClinicalTrials.gov, WHO ICTRP, ISRCTN, and CPCI-S to identify the relevant reports. We found 2419 records, but no studies addressed our initial question. Following advice from the WHO-Guideline committee and experts, we identified 6 manuscripts on allergy testing focusing on other populations showing that the prevalence of allergy confirmed by testing was low and the incidence of life-threatening reactions to BPG was very low (< 1-3/1000 individuals treated). A subsequent search addressed penicillin allergy delabeling. This found 516 records, and 5 studies addressing the safety of direct oral drug challenge vs. skin testing followed by drug administration in patients with suspected penicillin allergy. Immediate allergic reactions of minor severity were observed for a minority of patients and occurred less frequently in the direct drug challenge group: 2.3% vs. 11.5%; RR = 0.25, 95%CI 0.15-0.45, P < 0.00001, I2 = 0%. No anaphylaxis or deaths were observed. Severe allergic reactions to penicillin are extremely rare and can be recognized and dealt by trained healthcare workers. Confirmation of penicillin allergy diagnosis or delabeling using direct oral drug challenge or penicillin skin testing seems to be safe and is associated with a low rate of adverse reactions.
Keywords: Allergy; Penicillin; Rheumatic fever; Rheumatic heart disease.
© 2024. The Author(s).
Conflict of interest statement
The authors declared no competing interests.
Figures
References
-
- Revelas A, Taxmazidis O. Group A streptococcal infections in children. South Afr J Epidemiol Infect. 2012;27(3):98–103.
-
- Sika-Paotonu D, Beaton A, Raghu A et al (2016) Acute rheumatic fever and rheumatic heart disease. 2017 Mar 10 [Updated 2017 Apr 3]. In: Ferretti JJ, Stevens DL, Fischetti VA (eds) Streptococcus pyogenes: basic biology to clinical manifestations [Internet]. Oklahoma City (OK): University of Oklahoma Health Sciences Center; 2016-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK425394/
-
- World Health Organization (2018) Rheumatic fever and rheumatic heart disease: report by the Director-General. Seventy-first World Health Assembly. A71/25. Available at https://apps.who.int/gb/ebwha/pdf_files/WHA71/A71_25-en.pdf. Accessed 19 Feb 2024
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
