

Emerging Toxicities of Antibody-Drug Conjugates for Breast Cancer: Clinical Prioritization of Adverse Events from the FDA Adverse Event Reporting System
- PMID: 38696126
- PMCID: PMC11111510
- DOI: 10.1007/s11523-024-01058-9
Emerging Toxicities of Antibody-Drug Conjugates for Breast Cancer: Clinical Prioritization of Adverse Events from the FDA Adverse Event Reporting System
Abstract
Background: Antibody-drug conjugates (ADCs) are gaining widespread use in the treatment of breast cancer, although toxicity remains an underexplored issue in the real-world clinical setting. Individual case safety reports collected in large pharmacovigilance databases can advance our knowledge on their safety profile in routine clinical practice.
Objective: We prioritized adverse events (AEs) reported with ADCs approved for breast cancer using the Food and Drug Administration Adverse Event Reporting System (FAERS).
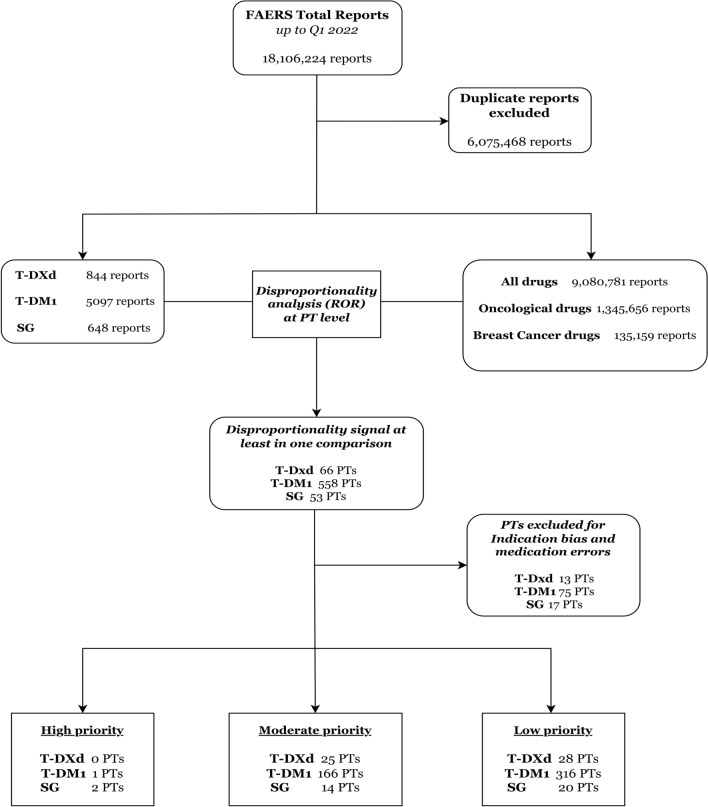
Methods: We assessed clinical priority of AEs reported in FAERS (February 2013-March 2022) for trastuzumab emtansine (T-DM1), trastuzumab deruxtecan (T-DXd), and sacituzumab govitecan (SG) by attributing a score to each AE disproportionally reported with ADCs. Four criteria were assessed: clinical relevance, reporting rate, reported case fatality rate, and stability of disproportionality signals (consistency of the reporting odds ratio across multiple analyses using three different comparators).
Results: We retained 6589 reports (77.4% referring to T-DM1 as suspect), and 572 AEs generated a disproportionality signal in at least one analysis. The majority of these AEs (62%) were classified as moderate clinical priorities (e.g., interstitial lung disease with T-DXd, thrombocytopenia, peripheral neuropathy with T-DM1, febrile neutropenia, and large intestine perforation with SG). Three AEs emerged as high clinical priorities (6 points): septic shock and neutropenic colitis with SG (N = 8 and 13, with median onset 13 and 10 days, respectively), without co-reported immunosuppressive agents; and pulmonary embolism with T-DM1 (N = 31, median onset 109 days, 52% with reported metastasis).
Conclusion: The heterogeneous spectrum of post-marketing toxicities for ADCs used in breast cancer, as emerging from the FAERS, is largely in line with preapproval evidence. Although causality cannot be proved, we call for increased awareness by oncologists on potential serious unexpected reactions, including early onset of septic shock and neutropenic colitis with SG, and late emergence of pulmonary embolism with T-DM1.
© 2024. The Author(s).
Conflict of interest statement
C.Z. has received grants from Novartis, Roche, Eisai, AstraZeneca, Pfizer, PharmaMar, Tesaro, Pierre Fabre, Ist. Gentili, Teva, Seagen, Eli Lilly, Celgene, MSD, GSK, Amgen, and Daiichi; has received support for attending meetings and/or travel from Novartis, Roche, Pfizer, PharmaMar, Tesaro, Pierre Fabre, Ist. Gentili, and Celgene; and has participated in data safety monitoring or advisory boards for Novartis, Roche, Eisai, AstraZeneca, Pfizer, PharmaMar, Amgen, Tesaro, Quintiles IMS, Eli Lilly, Celgene, MSD, GSK, and Daiichi. L.G. reports serving as a consultant/advisor for Lilly, Novartis, AstraZeneca, GlaxoSmithKline, and Incyte. S.C., S.P., M.F., M.Y., F.D.P., and E.R. have no conflicts of interest that are directly relevant to the content of this article.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
