

Dual energy for pulmonary vein isolation using dual-energy focal ablation technology integrated with a three-dimensional mapping system: SmartfIRE 3-month results
- PMID: 38696675
- PMCID: PMC11065353
- DOI: 10.1093/europace/euae088
Dual energy for pulmonary vein isolation using dual-energy focal ablation technology integrated with a three-dimensional mapping system: SmartfIRE 3-month results
Abstract
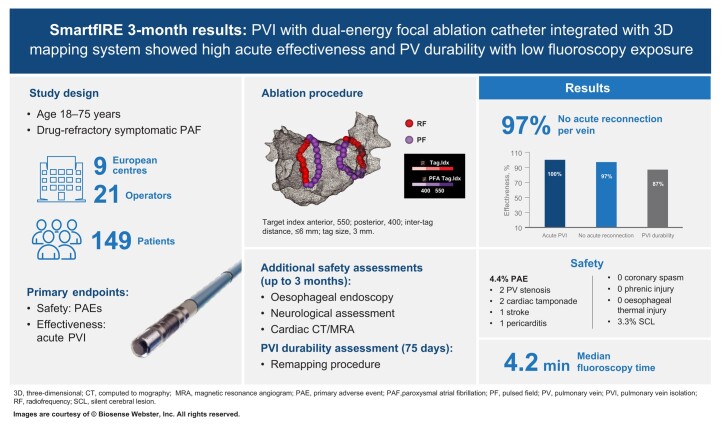
Aims: Contact force (CF)-sensing radiofrequency (RF) catheters with an ablation index have shown reproducible outcomes for the treatment of atrial fibrillation (AF) in large multicentre studies. A dual-energy (DE) focal CF catheter to deliver RF and unipolar/biphasic pulsed field ablation (PFA), integrated with a three-dimensional (3D) mapping system, can provide operators with additional flexibility. The SmartfIRE study assessed the safety and efficacy of this novel technology for the treatment of drug-refractory, symptomatic paroxysmal AF. Results at 3 months post-ablation are presented here.
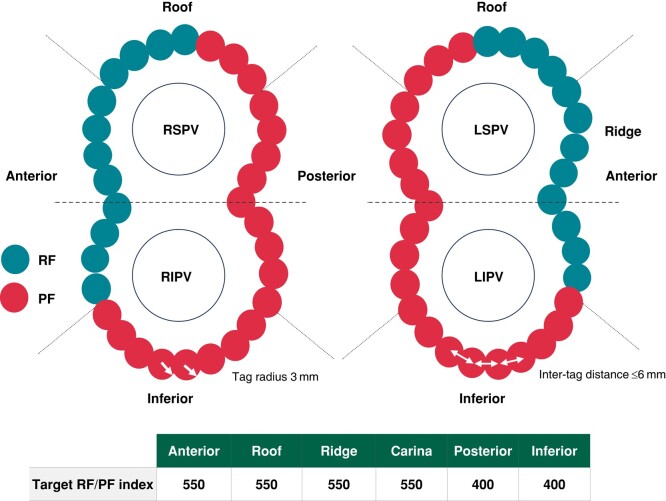
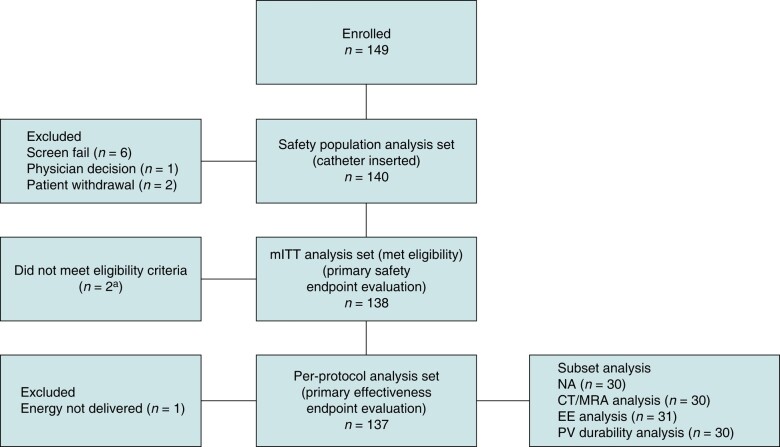
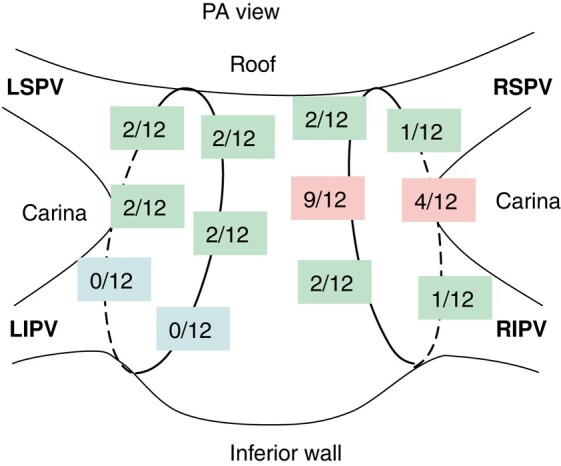
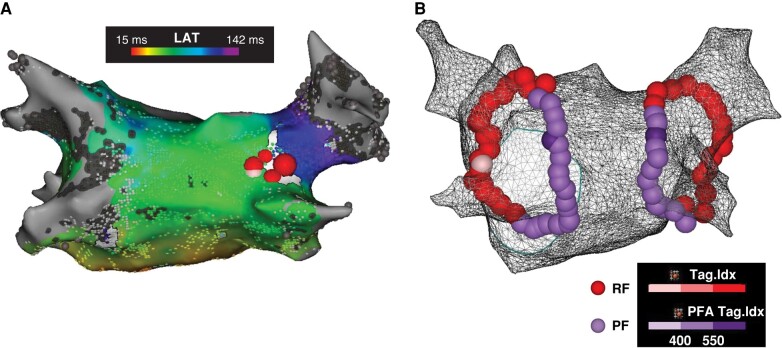
Methods and results: Pulmonary vein isolation (PVI) was performed using a DE focal, irrigated CF-sensing catheter with the recommendation of PFA at posterior/inferior and RF ablation at the anterior/ridge/carina segments. Irrespective of energy, a tag size of 3 mm; an inter-tag distance ≤6 mm; a target index of 550 for anterior, roof, ridge, and carina; and a target index of 400 for posterior and inferior were recommended. Cavotricuspid isthmus ablation was permitted in patients with documented typical atrial flutter. The primary effectiveness endpoint was acute procedural success. The primary safety endpoint was the rate of primary adverse events (PAEs) within 7 days of the procedure. A prespecified patient subset underwent oesophageal endoscopy (EE; 72 h post-procedure), neurological assessment (NA; pre-procedure and discharge), and cardiac computed tomography (CT)/magnetic resonance angiogram (MRA) imaging (pre-procedure and 3 months post-procedure) for additional safety evaluation, and a mandatory remapping procedure (Day 75 ± 15) for PVI durability assessment. Of 149 patients enrolled between February and June 2023, 140 had the study catheter inserted (safety analysis set) and 137 had ablation energy delivered (per-protocol analysis set). The median (Q1/Q3) total procedure and fluoroscopy times were 108.0 (91.0/126.0) and 4.2 (2.3/7.7) min (n = 137). The acute procedural success rate was 100%. First-pass isolation was achieved in 89.1% of patients and 96.8% of veins. Cavotricuspid isthmus ablations were successfully performed in 12 patients [pulsed field (PF) only: 6, RF only: 5, and RF/PF: 1]. The PAE rate was 4.4% [6/137 patients; 2 pulmonary vein (PV) stenoses, 2 cardiac tamponades/perforations, 1 stroke, and 1 pericarditis]. No coronary artery spasm was reported. No oesophageal lesion was seen in the EE subset (0/31, 0%). In the NA subset (n = 30), microemboli lesions were identified in 2 patients (2/30, 6.7%), both of which were resolved at follow-up; only 1 was symptomatic (silent cerebral lesion, 3.3%). In the CT/MRA subset (n = 30), severe PV narrowing (of >70%) was detected in 2 patients (2/30, 6.7%; vein level 2/128, 1.6%), of whom 1 underwent dilatation and stenting and 1 was asymptomatic; both were associated with high index values and a small inter-tag distance. In the PV durability subset (n = 30), 100/115 treated PVs (87%) were durably isolated and 18/30 patients (60.0%) had all PVs durably isolated.
Conclusion: A DE focal CF catheter with 3D mapping integration showed a 100% acute success rate with an acceptable safety profile in the treatment of paroxysmal AF. Prespecified 3-month remapping showed notable PVI durability.
Clinical trial registration: ClinicalTrials.gov Identifier: NCT05752487.
Keywords: Contact force catheter; Dual energy; Focal catheter; Pulmonary vein isolation; Pulsed field ablation; VISITAG SURPOINT.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: M.D. has served on the speakers bureau and as a consultant and has received research support from Biosense Webster, Inc. T.D.P. has received consulting fees and honoraria for lectures and presentations from Biosense Webster, Inc. and Adagio Medical (all payments were directed to institution). J.H. reports speakers fees and consultant honoraria from Biosense Webster, Inc. and Boston Scientific. T.P. reports support for attending a meeting and travel from Biosense Webster, Inc. J.V. reports research grants from Abbott, Biotronik, Boston Scientific, CardioFocus, and Medtronic; speakers fees from Abbott and CardioFocus; and serving on an advisory board for Boston Scientific. G.S. reports personal fees from Abbott, Bayer, Boston Scientific, Johnson & Johnson Medical, and LUMA Vision not related to the present study and fees from Johnson & Johnson Medical in relation to the present study. M.B.K. reports speakers fees from Biosense Webster, Inc. H.P. reports consultancy and honoraria as a speaker for Abbott, Biosense Webster, Inc., Boston Scientific, and Medtronic. P.L. has received consulting fees and a travel grant from Biosense Webster, Inc. outside the presented work. All remaining authors have declared no conflicts of interest.
Figures
References
-
- Joglar JA, Chung MK, Armbruster AL, Benjamin EJ, Chyou JY, Cronin EM et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024;149:e1–156. - PMC - PubMed
-
- Duytschaever M, Vijgen J, De Potter T, Scherr D, Van Herendael H, Knecht S et al. Standardized pulmonary vein isolation workflow to enclose veins with contiguous lesions: the multicentre VISTAX trial. Europace 2020;22:1645–52. - PubMed
-
- Di Biase L, Monir G, Melby D, Tabereaux P, Natale A, Manyam H et al. Composite index tagging for PVI in paroxysmal AF: a prospective, multicenter postapproval study. JACC Clin Electrophysiol 2022;8:1077–89. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
