

Constructing personalized characterizations of structural brain aberrations in patients with dementia using explainable artificial intelligence
- PMID: 38698139
- PMCID: PMC11066104
- DOI: 10.1038/s41746-024-01123-7
Constructing personalized characterizations of structural brain aberrations in patients with dementia using explainable artificial intelligence
Abstract
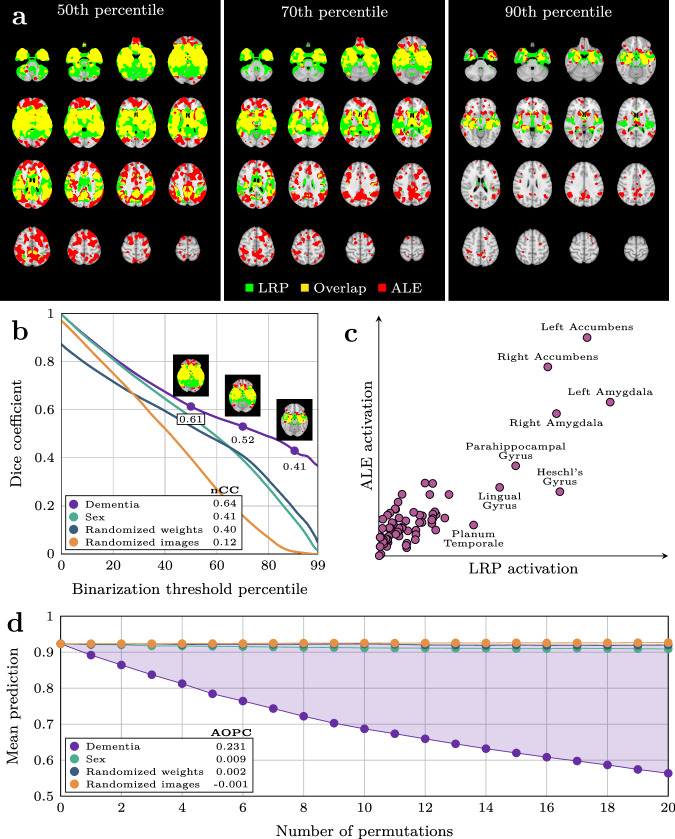
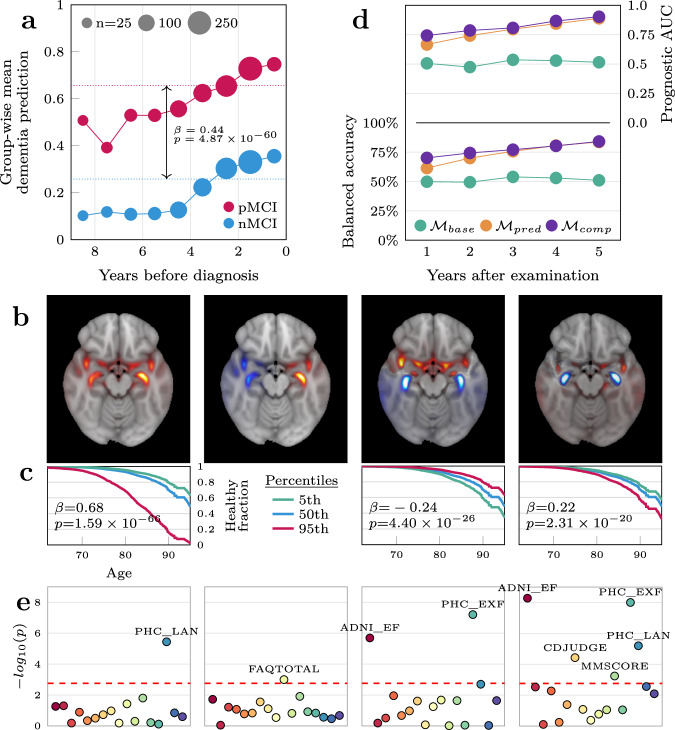
Deep learning approaches for clinical predictions based on magnetic resonance imaging data have shown great promise as a translational technology for diagnosis and prognosis in neurological disorders, but its clinical impact has been limited. This is partially attributed to the opaqueness of deep learning models, causing insufficient understanding of what underlies their decisions. To overcome this, we trained convolutional neural networks on structural brain scans to differentiate dementia patients from healthy controls, and applied layerwise relevance propagation to procure individual-level explanations of the model predictions. Through extensive validations we demonstrate that deviations recognized by the model corroborate existing knowledge of structural brain aberrations in dementia. By employing the explainable dementia classifier in a longitudinal dataset of patients with mild cognitive impairment, we show that the spatially rich explanations complement the model prediction when forecasting transition to dementia and help characterize the biological manifestation of disease in the individual brain. Overall, our work exemplifies the clinical potential of explainable artificial intelligence in precision medicine.
© 2024. The Author(s).
Conflict of interest statement
K.P. report work with Roche BN29553 and Novo Nordisk NN6535-4730 trials; All other authors declare that they have no competing interests.
Figures


References
Grants and funding
- 4MENT/University of Oslo | Livsvitenskap, Universitetet i Oslo (UiO:Life Science)
- 4MENT/University of Oslo | Livsvitenskap, Universitetet i Oslo (UiO:Life Science)
- 2019101/Ministry of Health and Care Services | Helse Sør-Øst RHF (Southern and Eastern Norway Regional Health Authority)
- Emmy Noether 513851350/Deutsche Forschungsgemeinschaft (German Research Foundation)
- 300767/Norges Forskningsråd (Research Council of Norway)
LinkOut - more resources
Full Text Sources
