

The causality of gut microbiota on onset and progression of sepsis: a bi-directional Mendelian randomization analysis
- PMID: 38698853
- PMCID: PMC11063379
- DOI: 10.3389/fimmu.2024.1266579
The causality of gut microbiota on onset and progression of sepsis: a bi-directional Mendelian randomization analysis
Abstract
Background: Several observational studies have proposed a potential link between gut microbiota and the onset and progression of sepsis. Nevertheless, the causality of gut microbiota and sepsis remains debatable and warrants more comprehensive exploration.
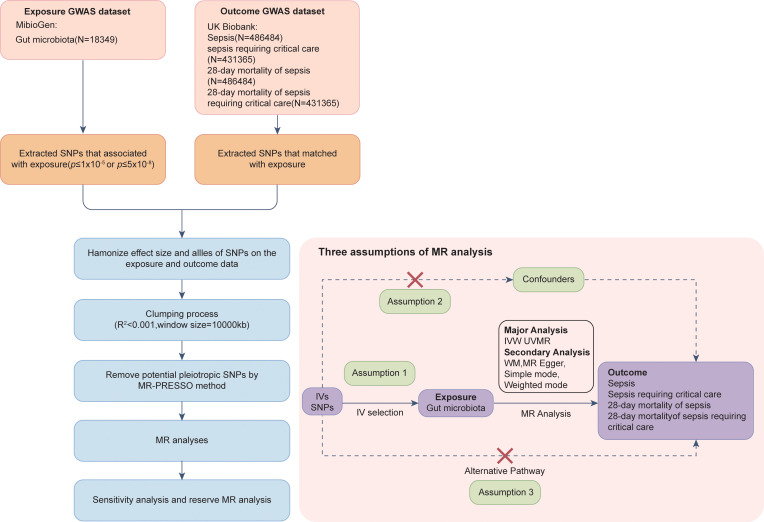
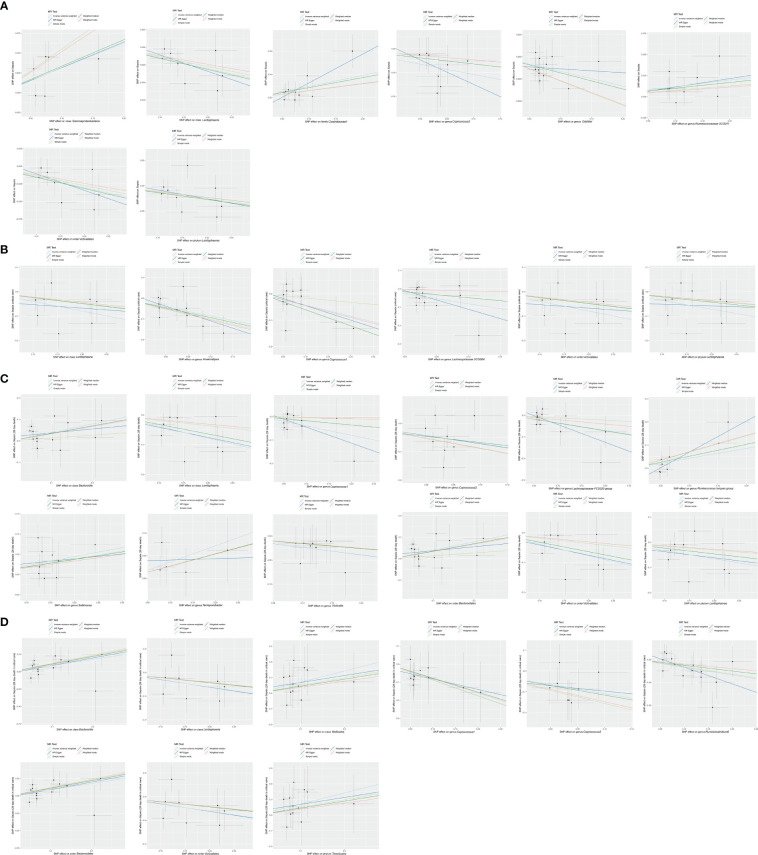
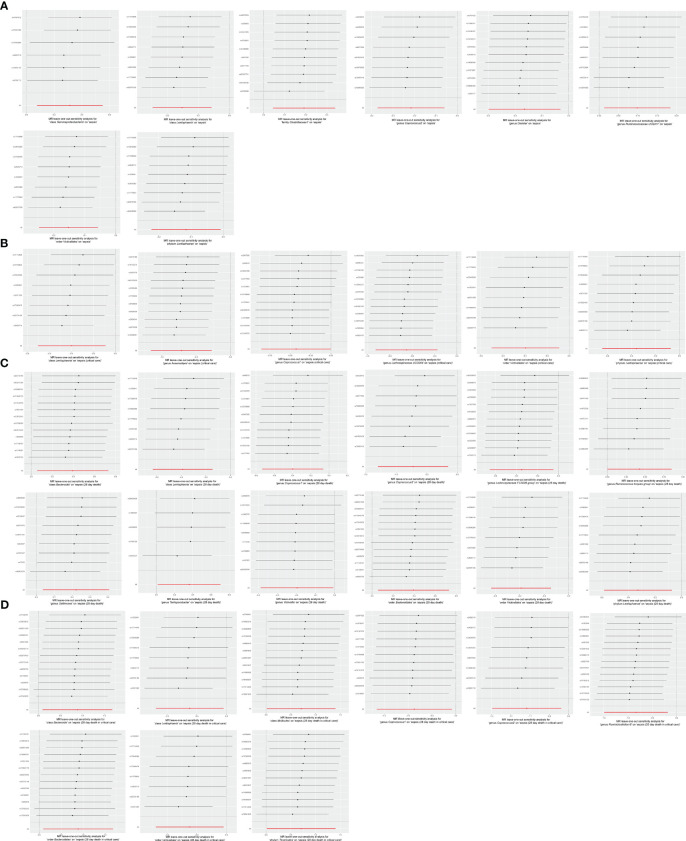
Methods: We conducted a two-sample Mendelian randomization (MR) analysis to test the causality between gut microbiota and the onset and progression of sepsis. The genome-wide association study (GWAS) summary statistics for 196 bacterial traits were extracted from the MiBioGen consortium, whereas the GWAS summary statistics for sepsis and sepsis-related outcomes came from the UK Biobank. The inverse-variance weighted (IVW) approach was the primary method used to examine the causal association. To complement the IVW method, we utilized four additional MR methods. We performed a series of sensitivity analyses to examine the robustness of the causal estimates.
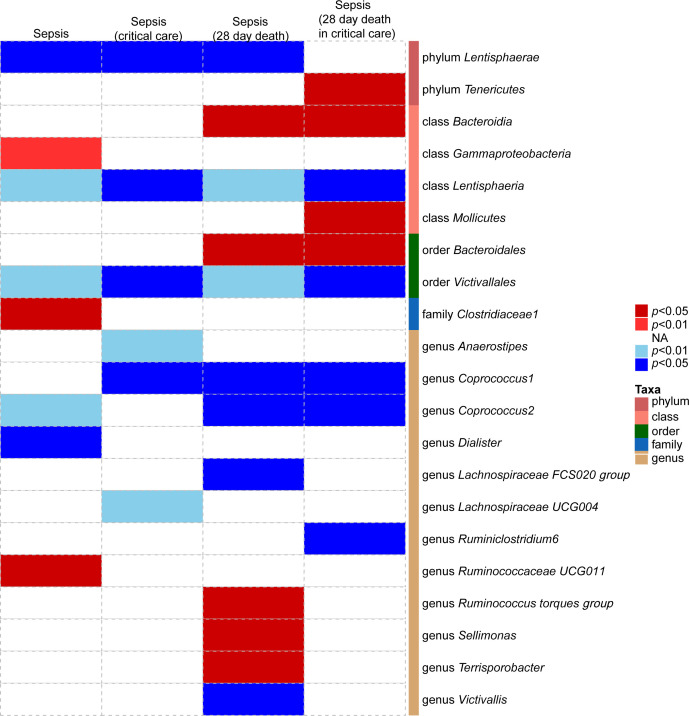
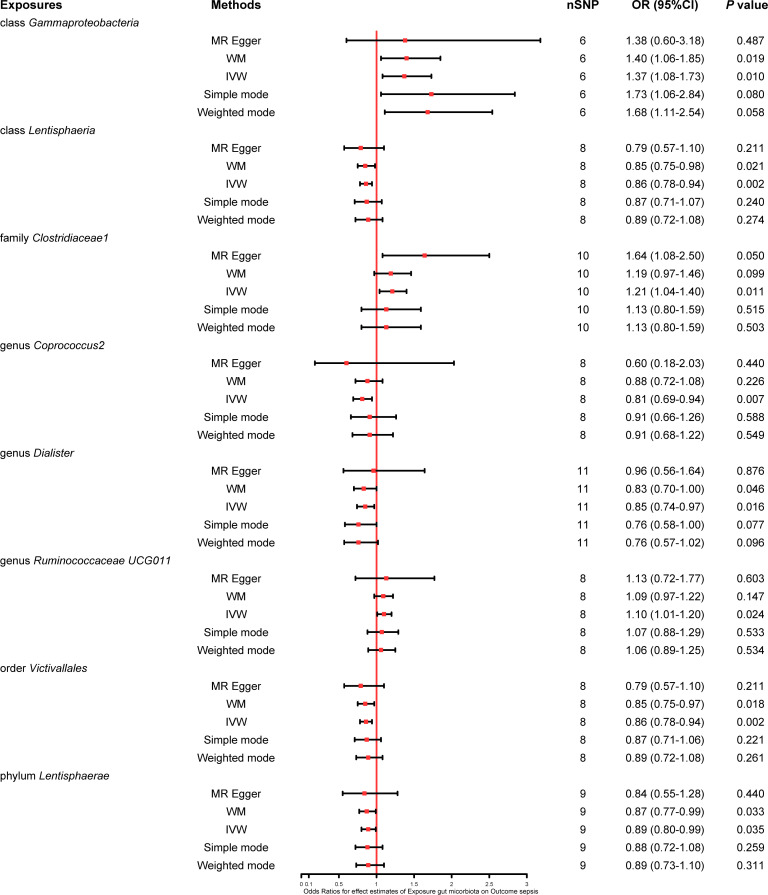
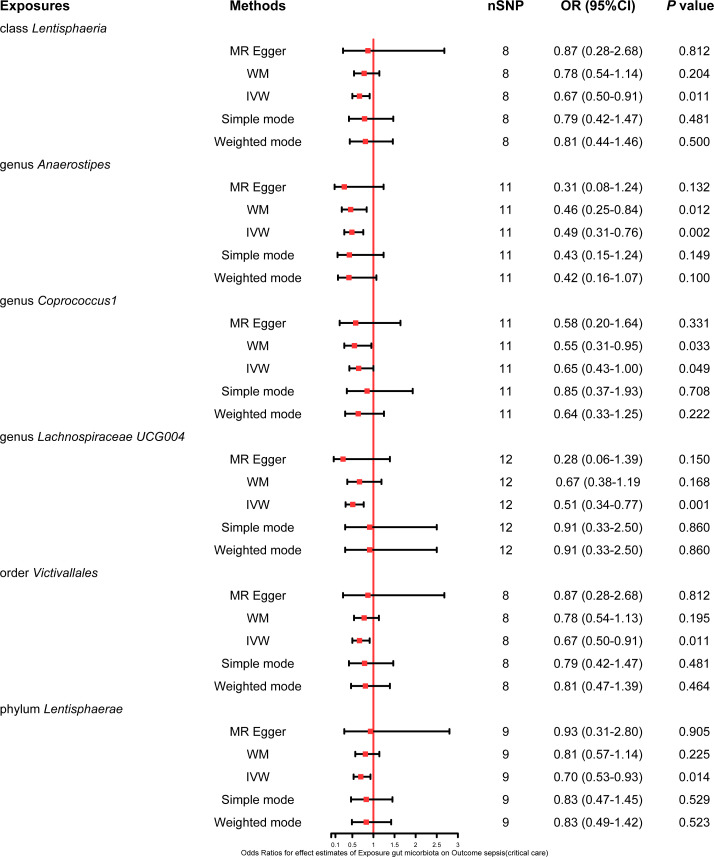
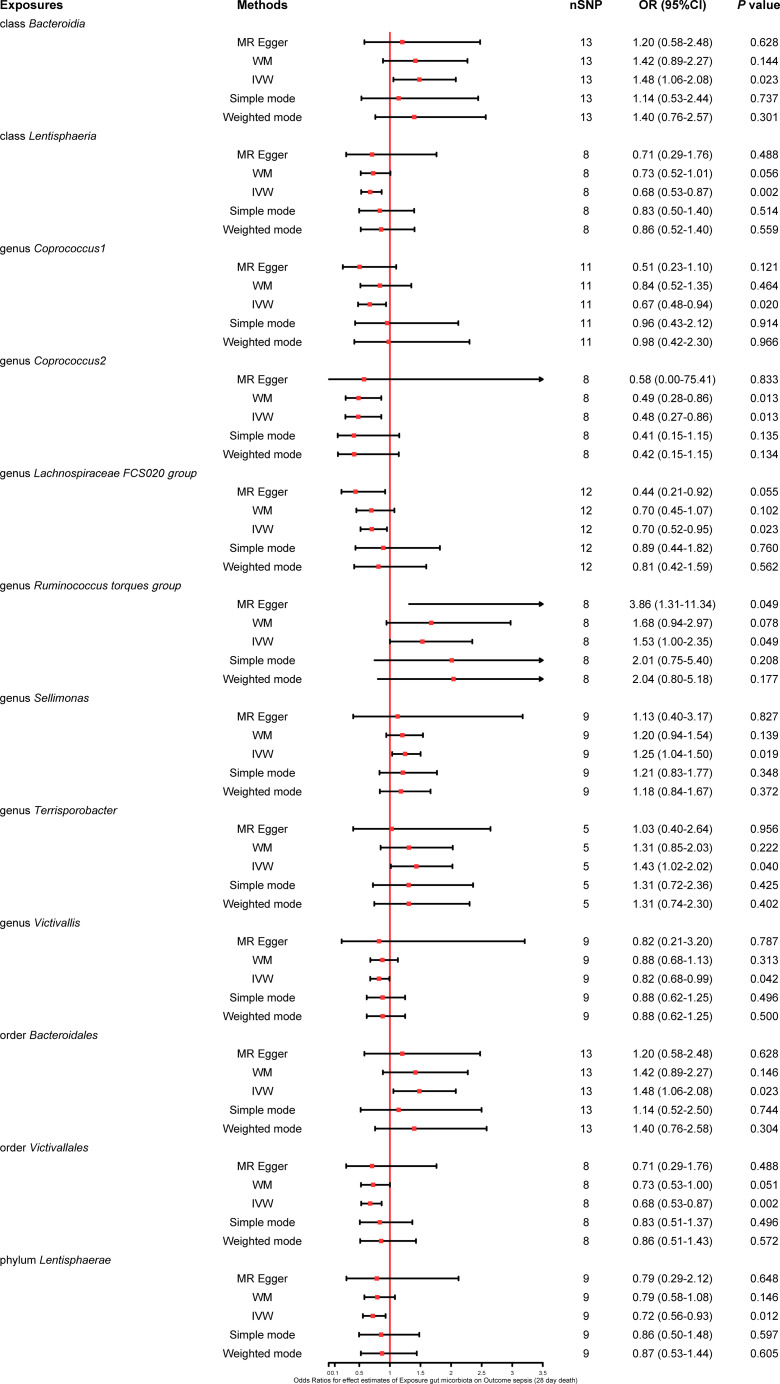
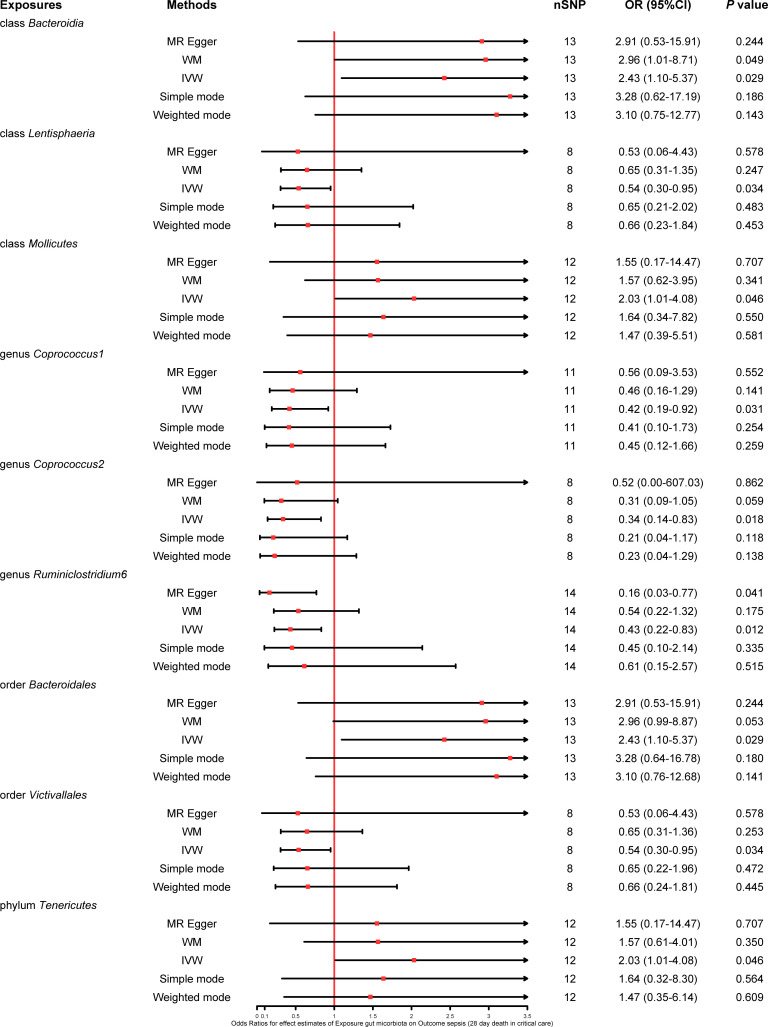
Results: We assessed the causality of 196 bacterial traits on sepsis and sepsis-related outcomes. Genus Coprococcus2 [odds ratio (OR) 0.81, 95% confidence interval (CI) (0.69-0.94), p = 0.007] and genus Dialister (OR 0.85, 95% CI 0.74-0.97, p = 0.016) had a protective effect on sepsis, whereas genus Ruminococcaceae UCG011 (OR 1.10, 95% CI 1.01-1.20, p = 0.024) increased the risk of sepsis. When it came to sepsis requiring critical care, genus Anaerostipes (OR 0.49, 95% CI 0.31-0.76, p = 0.002), genus Coprococcus1 (OR 0.65, 95% CI 0.43-1.00, p = 0.049), and genus Lachnospiraceae UCG004 (OR 0.51, 95% CI 0.34-0.77, p = 0.001) emerged as protective factors. Concerning 28-day mortality of sepsis, genus Coprococcus1 (OR 0.67, 95% CI 0.48-0.94, p = 0.020), genus Coprococcus2 (OR 0.48, 95% CI 0.27-0.86, p = 0.013), genus Lachnospiraceae FCS020 (OR 0.70, 95% CI 0.52-0.95, p = 0.023), and genus Victivallis (OR 0.82, 95% CI 0.68-0.99, p = 0.042) presented a protective effect, whereas genus Ruminococcus torques group (OR 1.53, 95% CI 1.00-2.35, p = 0.049), genus Sellimonas (OR 1.25, 95% CI 1.04-1.50, p = 0.019), and genus Terrisporobacter (OR 1.43, 95% CI 1.02-2.02, p = 0.040) presented a harmful effect. Furthermore, genus Coprococcus1 (OR 0.42, 95% CI 0.19-0.92, p = 0.031), genus Coprococcus2 (OR 0.34, 95% CI 0.14-0.83, p = 0.018), and genus Ruminiclostridium6 (OR 0.43, 95% CI 0.22-0.83, p = 0.012) were associated with a lower 28-day mortality of sepsis requiring critical care.
Conclusion: This MR analysis unveiled a causality between the 21 bacterial traits and sepsis and sepsis-related outcomes. Our findings may help the development of novel microbiota-based therapeutics to decrease the morbidity and mortality of sepsis.
Keywords: Mendelian randomization; causal relationship; genetics; gut microbiota; sepsis.
Copyright © 2024 Gao, Liu, Cui, Zhang and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Gut microbiota and sepsis and sepsis-related death: a Mendelian randomization investigation.Front Immunol. 2024 Jan 31;15:1266230. doi: 10.3389/fimmu.2024.1266230. eCollection 2024. Front Immunol. 2024. PMID: 38361921 Free PMC article.
-
Genetic support of the causal association between gut microbiota and peripheral artery disease: a bidirectional Mendelian randomization study.Aging (Albany NY). 2024 Jan 9;16(1):762-778. doi: 10.18632/aging.205417. Epub 2024 Jan 9. Aging (Albany NY). 2024. PMID: 38198148 Free PMC article.
-
Causal associations between gut microbiota and premature rupture of membranes: a two-sample Mendelian randomization study.Front Immunol. 2024 Sep 2;15:1440232. doi: 10.3389/fimmu.2024.1440232. eCollection 2024. Front Immunol. 2024. PMID: 39286243 Free PMC article.
-
Genetic liability of gut microbiota for idiopathic pulmonary fibrosis and lung function: a two-sample Mendelian randomization study.Front Cell Infect Microbiol. 2024 May 22;14:1348685. doi: 10.3389/fcimb.2024.1348685. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38841114 Free PMC article.
-
Exploring the potential causal relationship between gut microbiota and heart failure: A two-sample mendelian randomization study combined with the geo database.Curr Probl Cardiol. 2024 Feb;49(2):102235. doi: 10.1016/j.cpcardiol.2023.102235. Epub 2023 Nov 30. Curr Probl Cardiol. 2024. PMID: 38040216 Review.
Cited by
-
Genetically Predicted Peripheral Immune Cells Mediate the Effect of Gut Microbiota on Influenza Susceptibility.Int J Mol Sci. 2024 Jul 14;25(14):7706. doi: 10.3390/ijms25147706. Int J Mol Sci. 2024. PMID: 39062949 Free PMC article.
-
Causal effect of gut microbiota on venous thromboembolism: a two-sample mendelian randomization study.Thromb J. 2024 Nov 29;22(1):106. doi: 10.1186/s12959-024-00676-7. Thromb J. 2024. PMID: 39614282 Free PMC article.
-
Causal association between gastroesophageal reflux disease and sepsis, and the mediating role of gut bacterial abundance, a Mendelian randomization study.Medicine (Baltimore). 2025 Feb 21;104(8):e41631. doi: 10.1097/MD.0000000000041631. Medicine (Baltimore). 2025. PMID: 39993106 Free PMC article.
References
-
- Fleischmann-Struzek C, Mellhammar L, Rose N, Cassini A, Rudd KE, Schlattmann P, et al. . Incidence and mortality of hospital- and ICU-treated sepsis: results from an updated and expanded systematic review and meta-analysis. Intensive Care Med. (2020) 46:1552–62. doi: 10.1007/s00134-020-06151-x - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical