

Prevalence and clinical markers of herpes simplex virus infection in oral lesions of bullous pemphigoid
- PMID: 38698862
- PMCID: PMC11063318
- DOI: 10.3389/fimmu.2024.1387503
Prevalence and clinical markers of herpes simplex virus infection in oral lesions of bullous pemphigoid
Abstract
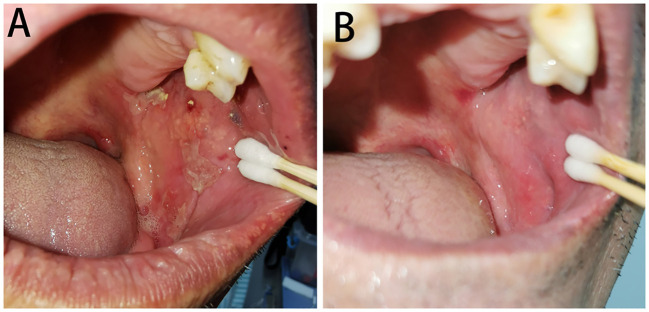
Background: The manifestations of bullous pemphigoid (BP) and herpes simplex virus (HSV) infection are similar in oral mucosa, and the laboratory detection of HSV has some limitations, making it difficult to identify the HSV infection in oral lesions of BP. In addition, the treatments for BP and HSV infection have contradictory aspects. Thus, it is important to identify the HSV infection in BP patients in time.
Objective: To identify the prevalence and clinical markers of HSV infection in oral lesions of BP.
Methods: This prospective cross-sectional descriptive analytical study was conducted on 42 BP patients with oral lesions. A total of 32 BP patients without oral lesions and 41 healthy individuals were enrolled as control groups. Polymerase chain reaction was used to detect HSV. Clinical and laboratory characteristics of patients with HSV infection were compared with those without infection.
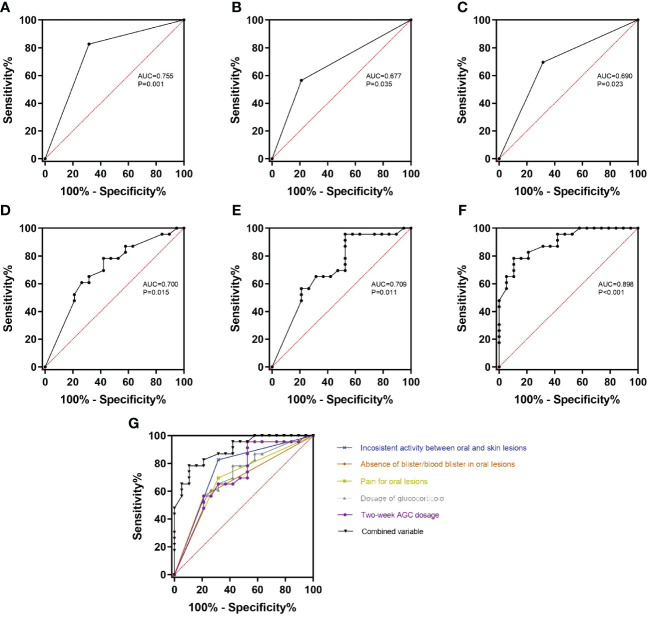
Results: A total of 19 (45.2%) BP patients with oral lesions, none (0.0%) BP patients without oral lesions, and four (9.8%) healthy individuals were positive for HSV on oral mucosa. Among BP patients with oral lesions, the inconsistent activity between oral and skin lesions (p=0.001), absence of blister/blood blister in oral lesions (p=0.020), and pain for oral lesions (p=0.014) were more often seen in HSV-positive than HSV-negative BP patients; the dosage of glucocorticoid (p=0.023) and the accumulated glucocorticoid dosage in the last 2 weeks (2-week AGC dosage) (p=0.018) were higher in HSV-positive BP patients. Combining the above five variables as test variable, the AUC was 0.898 (p<0.001) with HSV infection as state variable in ROC analysis. The absence of blister/blood blister in oral lesions (p=0.030) and pain for oral lesions (p=0.038) were found to be independent predictors of HSV infection in multivariable analysis. A total of 14 (73.7%) HSV-positive BP patients were treated with 2-week famciclovir and the oral mucosa BPDAI scores significantly decreased (p<0.001).
Conclusion: HSV infection is common in BP oral lesions. The inconsistent activity between oral and skin lesions, absence of blister in oral lesions, pain for oral lesions, higher currently used glucocorticoid dosage, and higher 2-week AGC dosage in BP patients should alert physicians to HSV infection in oral lesions and treat them with 2-week famciclovir in time.
Keywords: Bullous pemphigoid; HSV; autoimmune subepidermal bullous disease; clinical markers; infection; oral lesions; prevalence.
Copyright © 2024 Zhang, Yu, Liang, Li, Zhao, Jing and Feng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Occult herpes simplex virus colonization of bullous dermatitides.Am J Clin Dermatol. 2008;9(3):163-8. doi: 10.2165/00128071-200809030-00004. Am J Clin Dermatol. 2008. PMID: 18429645
-
Features of oral, pharyngeal, and laryngeal lesions in bullous pemphigoid.Ear Nose Throat J. 2016 Oct-Nov;95(10-11):E1-E5. Ear Nose Throat J. 2016. PMID: 27792825
-
Mucosal Involvement in Bullous Pemphigoid Is Mostly Associated with Disease Severity and to Absence of Anti-BP230 Autoantibody.Front Immunol. 2018 Mar 13;9:479. doi: 10.3389/fimmu.2018.00479. eCollection 2018. Front Immunol. 2018. PMID: 29662486 Free PMC article. Clinical Trial.
-
[Bullous autoimmune diseases of the oral mucosa].Rev Stomatol Chir Maxillofac. 1999 Oct;100(5):230-9. Rev Stomatol Chir Maxillofac. 1999. PMID: 10604215 Review. French.
-
Autoimmune Subepidermal Bullous Diseases of the Skin and Mucosae: Clinical Features, Diagnosis, and Management.Clin Rev Allergy Immunol. 2018 Feb;54(1):26-51. doi: 10.1007/s12016-017-8633-4. Clin Rev Allergy Immunol. 2018. PMID: 28779299 Review.
Cited by
-
Development and Evaluation of the Biological Activities of a Plain Mucoadhesive Hydrogel as a Potential Vehicle for Oral Mucosal Drug Delivery.Gels. 2024 Sep 3;10(9):574. doi: 10.3390/gels10090574. Gels. 2024. PMID: 39330176 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical