

Derivation and internal validation of the multivariate toxigenic C. difficile diarrhea model and risk score for emergency room and hospitalized patients with diarrhea
- PMID: 38698945
- PMCID: PMC11062795
- DOI: 10.1017/ash.2024.58
Derivation and internal validation of the multivariate toxigenic C. difficile diarrhea model and risk score for emergency room and hospitalized patients with diarrhea
Abstract
Background: Many factors have been associated with the risk of toxigenic C. difficile diarrhea (TCdD). This study derived and internally validated a multivariate model for estimating the risk of TCdD in patients with diarrhea using readily available clinical factors.
Methods: A random sample of 3,050 symptomatic emergency department or hospitalized patients undergoing testing for toxigenic C. difficile at a single teaching hospital between 2014 and 2018 was created. Unformed stool samples positive for both glutamate dehydrogenase antigen by enzyme immunoassay and tcdB gene by polymerase chain reaction were classified as TCdD positive. The TCdD Model was created using logistic regression and was modified to the TCdD Risk Score to facilitate its use.
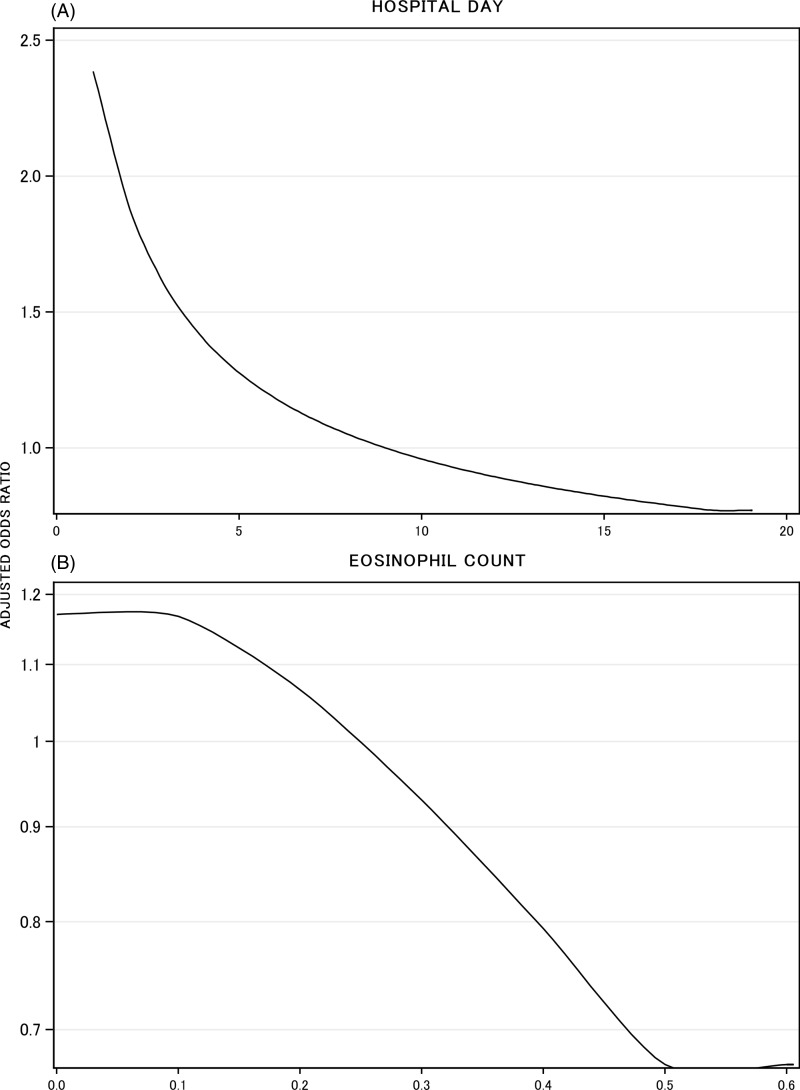
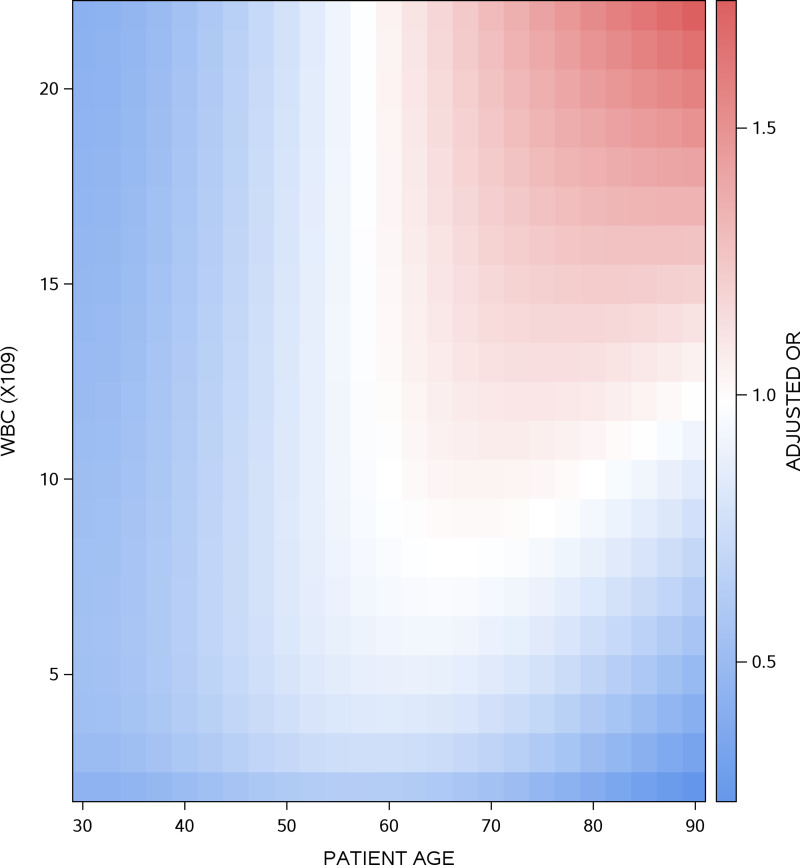
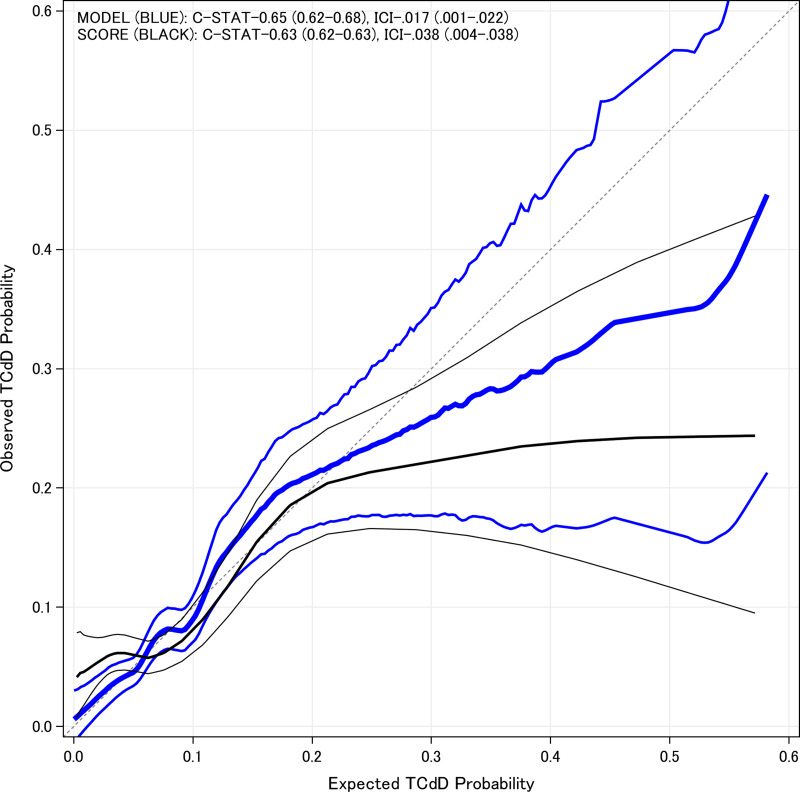
Results: 8.1% of patients were TCdD positive. TCdD risk increased with abdominal pain (adjusted odds ratio 1.3; 95% CI, 1.0-1.8), previous C. difficile diarrhea (2.5, 1.1-6.1), and prior antibiotic exposure, especially when sampled in the emergency department (4.2, 2.5-7.0) versus the hospital (1.7, 1.3-2.3). TCdD risk also increased when testing occurred earlier during the hospitalization encounter, when age and white cell count increased concurrently, and with decreased eosinophil count. In internal validation, the TCdD Model had moderate discrimination (optimism-corrected C-statistic 0.65, 0.62-0.68) and good calibration (optimism-corrected Integrated Calibration Index [ICI] 0.017, 0.001-0.022). Performance decreased slightly for the TCdD Risk Score (C-statistic 0.63, 0.62-0.63; ICI 0.038, 0.004-0.038).
Conclusions: TCdD risk can be predicted using readily available clinical risk factors with modest accuracy.
© Published by Cambridge University Press 2024.
Conflict of interest statement
The authors have no conflicts of interest and no funding was received for the study.
Figures
References
-
- Karas JA, Enoch DA, Aliyu SH. A review of mortality due to Clostridium difficile infection. J Infect 2010;61:1–8. - PubMed
-
- Deshpande A, Pasupuleti V, Thota P, et al. Risk factors for recurrent Clostridium difficile infection: a systematic review and meta-analysis. Infect Control Hosp Epidemiol 2015;36:452–460. - PubMed
LinkOut - more resources
Full Text Sources