

Endovascular thrombectomy is cost-saving in patients with acute ischemic stroke with large infarct
- PMID: 38699058
- PMCID: PMC11064842
- DOI: 10.3389/fneur.2024.1324074
Endovascular thrombectomy is cost-saving in patients with acute ischemic stroke with large infarct
Abstract
Objective: Endovascular thrombectomy (EVT) is the standard of care for acute large vessel occlusion stroke. Recently, the ANGEL-ASPECT and SELECT 2 trials showed improved outcomes in patients with acute ischemic Stroke presenting with large infarcts. The cost-effectiveness of EVT for this subpopulation of stroke patients has only been calculated using data from the previously published RESCUE-Japan LIMIT trial. It is, therefore, limited in its generalizability to an international population. With this study we primarily simulated patient-level costs to analyze the economic potential of EVT for patients with large ischemic stroke from a public health payer perspective based on the recently published data and secondarily identified determinants of cost-effectiveness.
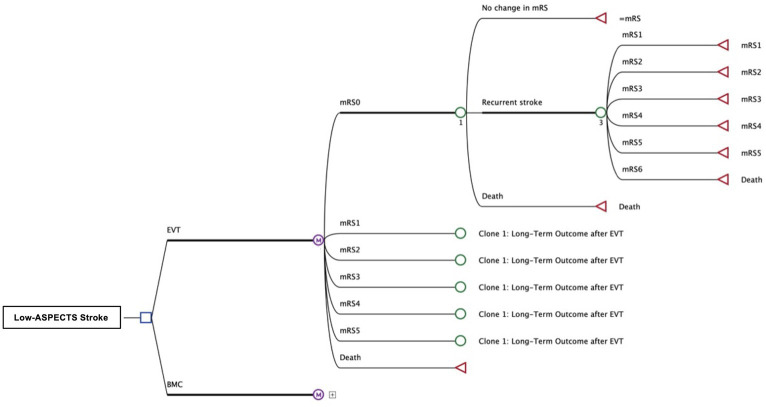
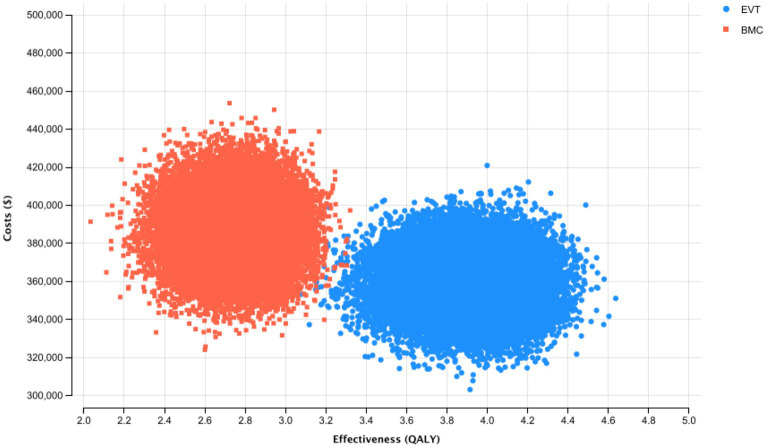
Methods: Costs and outcome of patients treated with EVT or only with the best medical care based on the recent prospective clinical trials ANGEL-ASPECT, SELECT2 and RESCUE-Japan LIMIT. A A Markov model was developed using treamtment outcomes derived from the most recent available literature. Deterministic and probabilistic sensitivity analyses addressed uncertainty.
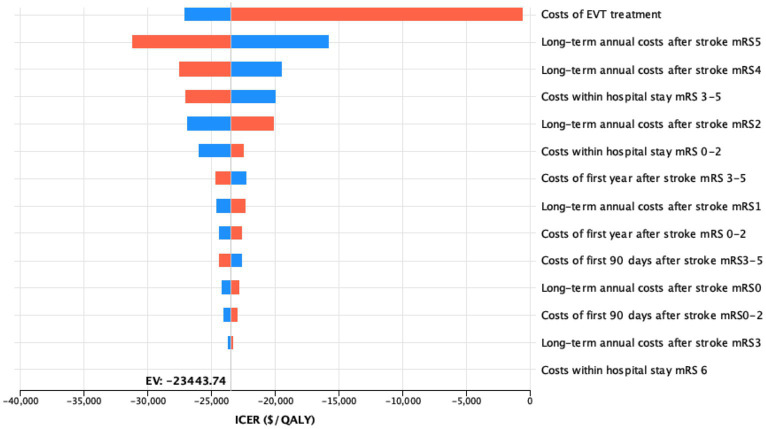
Results: Endovascular treatment resulted in an incremental gain of 1.32 QALYs per procedure with cost savings of $17,318 per patient. Lifetime costs resulted to be most sensitive to the costs of the endovascular procedure.
Conclusion: EVT is a cost-saving (i.e., dominant) strategy for patients presenting with large ischemic cores defined by inclusion criteria of the recently published ANGEL-ASPECT, SELECT2, and RESCUE-Japan LIMIT trials in comparison to best medical care in our simulation. Prospective data of individual patients need to be collected to validate these results.
Keywords: ASPECT score; cost-effectiveness; endovascular treatment; stroke; thrombectomy.
Copyright © 2024 Schwarting, Froelich, Kirschke, Mehrens, Bodden, Sepp, Reis, Dimitriadis, Ricke, Zimmer, Boeckh-Behrens and Kunz.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Cost-effectiveness of endovascular thrombectomy with alteplase versus endovascular thrombectomy alone for acute ischemic stroke secondary to large vessel occlusion.CMAJ Open. 2023 May 16;11(3):E443-E450. doi: 10.9778/cmajo.20220096. Print 2023 May-Jun. CMAJ Open. 2023. PMID: 37192770 Free PMC article.
-
Endovascular thrombectomy in patients with large core ischemic stroke: a cost-effectiveness analysis from the SELECT study.J Neurointerv Surg. 2021 Oct;13(10):875-882. doi: 10.1136/neurintsurg-2020-016766. Epub 2020 Nov 13. J Neurointerv Surg. 2021. PMID: 33188155
-
Cost-effectiveness of Endovascular Treatment for Acute Stroke with Large Infarct: A United States Perspective.Radiology. 2023 Oct;309(1):e223320. doi: 10.1148/radiol.223320. Radiology. 2023. PMID: 37787675 Clinical Trial.
-
Is Endovascular Therapy for Stroke Cost-Effective Globally? A Systematic Review of the Literature.J Stroke Cerebrovasc Dis. 2021 Apr;30(4):105557. doi: 10.1016/j.jstrokecerebrovasdis.2020.105557. Epub 2021 Feb 5. J Stroke Cerebrovasc Dis. 2021. PMID: 33556672
-
Cost-effectiveness analysis of endovascular treatment with or without intravenous thrombolysis in acute ischemic stroke.J Neurosurg. 2022 Jun 10;138(1):223-232. doi: 10.3171/2022.4.JNS22514. Print 2023 Jan 1. J Neurosurg. 2022. PMID: 35901768 Review.
Cited by
-
Intra-Arterial Deoxyribonuclease Therapy Improves Stroke Outcomes in Aged Mice.CNS Neurosci Ther. 2025 Jun;31(6):e70461. doi: 10.1111/cns.70461. CNS Neurosci Ther. 2025. PMID: 40457526 Free PMC article.
References
LinkOut - more resources
Full Text Sources