

Caffeine intake enhances bowel recovery after colorectal surgery: a meta-analysis of randomized and non-randomized studies
- PMID: 38700642
- PMCID: PMC11129976
- DOI: 10.1007/s13304-024-01847-x
Caffeine intake enhances bowel recovery after colorectal surgery: a meta-analysis of randomized and non-randomized studies
Abstract
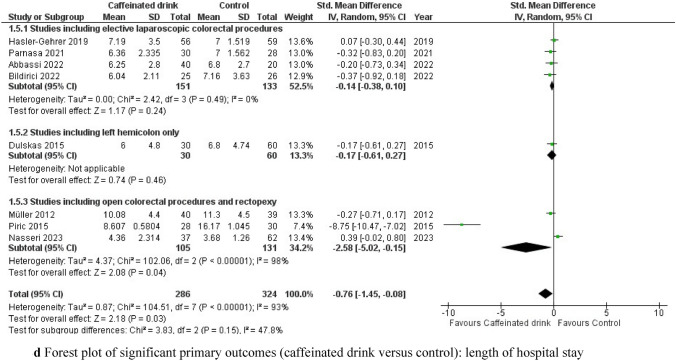
Postoperative ileus (POI) after colorectal surgery is a major problem that affects both patient recovery and hospital costs highlighting the importance of preventive strategies. Therefore, we aimed to perform a systematic analysis of the effects of postoperative caffeine consumption on bowel recovery and surgical morbidity after colorectal surgery. A comprehensive literature search was conducted through September 2023 for randomized and non-randomized trials comparing the effect of caffeinated versus non-caffeinated drinks on POI by evaluating bowel movement resumption, time to first flatus and solid food intake, and length of hospital stay (LOS). Secondary outcome analysis included postoperative morbidity in both groups. After data extraction and inclusion in a meta-analysis, odds ratios (ORs) for dichotomous variables and standardized mean differences (SMDs) for continuous outcomes with 95% confidence intervals (CIs) were calculated. Subgroup analyses were performed in cases of substantial heterogeneity. Six randomized and two non-randomized trials with a total of 610 patients were included in the meta-analysis. Caffeine intake significantly reduced time to first bowel movement [SMD -0.39, (95% CI -0.66 to -0.12), p = 0.005] and time to first solid food intake [SMD -0.41, (95% CI -0.79 to -0.04), p = 0.03] in elective laparoscopic colorectal surgery, while time to first flatus, LOS, and the secondary outcomes did not differ significantly. Postoperative caffeine consumption may be a reasonable strategy to prevent POI after elective colorectal surgery. However, larger randomized controlled trials (RCTs) with homogeneous study protocols, especially regarding the dosage form of caffeine and coffee, are needed.
Keywords: Caffeine intake; Coffee intake; Colorectal surgery; Postoperative complications; Postoperative ileus.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
