

Laparoscopic excision of accessory spleen for recurrent autoimmune hemolytic anemia after splenectomy: a case report
- PMID: 38700738
- PMCID: PMC11068696
- DOI: 10.1186/s40792-024-01884-z
Laparoscopic excision of accessory spleen for recurrent autoimmune hemolytic anemia after splenectomy: a case report
Abstract
Background: Splenectomy is indicated in cases of autoimmune hemolytic anemia (AIHA), which are refractory to medical management. In post-splenectomy, there exists a theoretical risk of AIHA recurrence, especially if an accessory spleen undergoes compensatory hypertrophy. In this context, we present a unique case of recurrent AIHA managed through laparoscopic excision of the accessory spleen (LEAS).
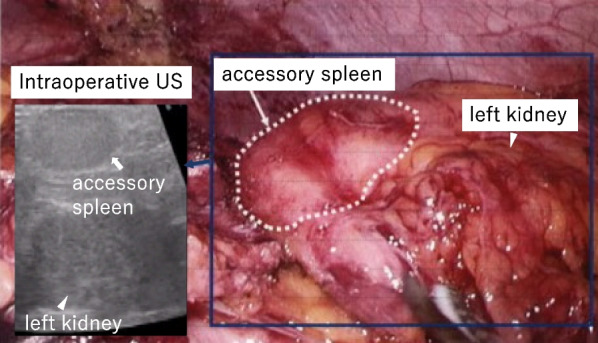
Case presentation: A 60-year-old male underwent laparoscopic splenectomy (LS) for AIHA refractory to standard medical therapies. Following the surgery, there was a marked improvement in hemolytic anemia symptoms, and oral steroid therapy was terminated 7 months post-LS. Nonetheless, a year after the LS, the patient exhibited a marked decline in hemoglobin levels, dropping to a concerning 5.8 g/dl, necessitating the reintroduction of oral steroids. A subsequent contrast-enhanced computed tomography (CT) scan unveiled an enlarged accessory spleen. The patient then underwent LEAS, during which the accessory spleen, obscured within adipose tissue, proved challenging to visualize laparoscopically. This obstacle was surmounted utilizing intraoperative ultrasonography (US), enabling successful excision of the accessory spleen. The post-surgical period progressed without complications, and the steroid dosage was reduced to one-twelfth of its initial preoperative quantity.
Conclusions: Recurrent AIHA can be instigated by post-splenectomy compensatory hypertrophy of the accessory spleen. Ensuring comprehensive splenic tissue excision is crucial in AIHA management to obviate recurrent stemming from hypertrophic remnants. In scenarios of AIHA recurrence tied to an enlarged accessory spleen, LEAS stands as a viable and effective therapeutic modality.
Keywords: AIHA; Autoimmune hemolytic anemia; Intraoperative ultrasonography; Laparoscopic excision of accessory spleen.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Laparoscopic excision of accessory spleen.Am J Surg. 2000 Jul;180(1):62-4. doi: 10.1016/s0002-9610(00)00417-7. Am J Surg. 2000. PMID: 11036144
-
Laparoscopic accessory splenectomy: the value of perioperative localization studies.Surg Endosc. 2009 Dec;23(12):2675-9. doi: 10.1007/s00464-008-0258-5. Epub 2009 Jan 23. Surg Endosc. 2009. PMID: 19165541
-
Computed tomography to detect accessory spleens before laparoscopic splenectomy: is it necessary?Surg Endosc. 2011 Jan;25(1):261-5. doi: 10.1007/s00464-010-1171-2. Epub 2010 Jun 22. Surg Endosc. 2011. PMID: 20567847
-
The Role of the Spleen and the Place of Splenectomy in Autoimmune Hemolytic Anemia-A Review of Current Knowledge.Diagnostics (Basel). 2023 Sep 9;13(18):2891. doi: 10.3390/diagnostics13182891. Diagnostics (Basel). 2023. PMID: 37761258 Free PMC article. Review.
-
Laparoscopic surgery of the spleen: state of the art.Langenbecks Arch Surg. 2001 Apr;386(3):230-9. doi: 10.1007/s004230100222. Langenbecks Arch Surg. 2001. PMID: 11382327 Review.
References
-
- Casaccia M, Torelli P, Squarcia S, Sormani MP, Savelli A, Troilo B, et al. Laparoscopic splenectomy for hematologic diseases: a preliminary analysis performed on the Italian Registry of Laparoscopic Surgery of the Spleen (IRLSS) Surg Endosc. 2006;20(8):1214–1220. doi: 10.1007/s00464-005-0527-5. - DOI - PubMed
-
- Gigot JF, Jamar F, Ferrant A, van Beers BE, Lengele B, Pauwels S, et al. Inadequate detection of accessory spleens and splenosis with laparoscopic splenectomy. A shortcoming of the laparoscopic approach in hematologic diseases. Surg Endosc. 1998;12(2):101–106. doi: 10.1007/s004649900607. - DOI - PubMed
LinkOut - more resources
Full Text Sources
