

Competing risks of monomorphic vs. non-monomorphic ventricular arrhythmias in primary prevention implantable cardioverter-defibrillator recipients: Global Electrical Heterogeneity and Clinical Outcomes (GEHCO) study
- PMID: 38703375
- PMCID: PMC11167666
- DOI: 10.1093/europace/euae127
Competing risks of monomorphic vs. non-monomorphic ventricular arrhythmias in primary prevention implantable cardioverter-defibrillator recipients: Global Electrical Heterogeneity and Clinical Outcomes (GEHCO) study
Abstract
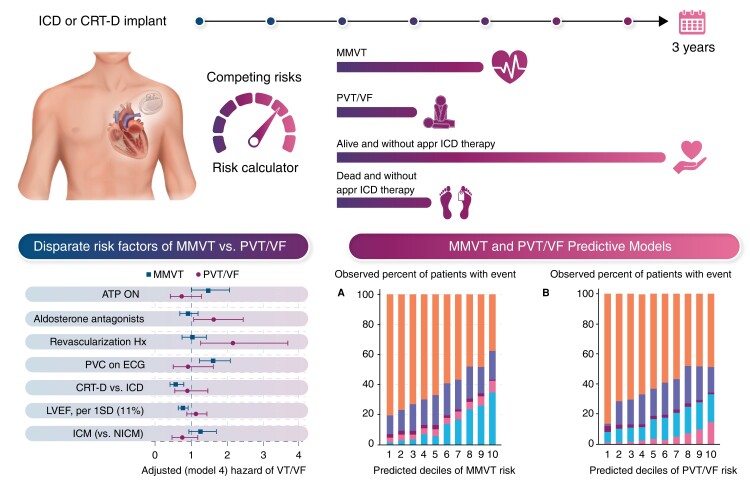
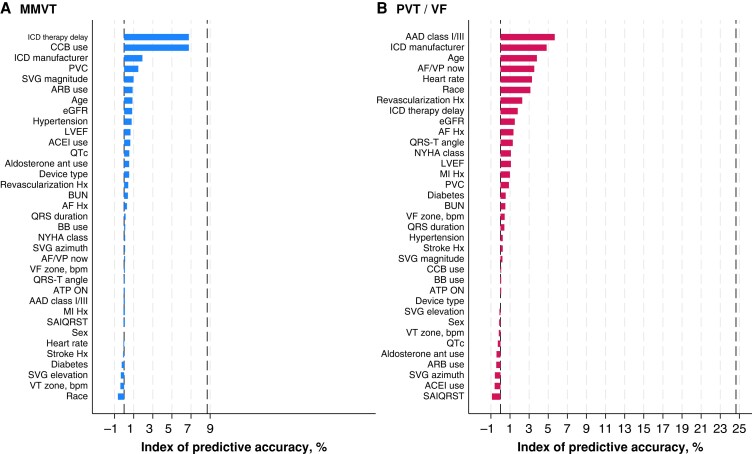
Aims: Ablation of monomorphic ventricular tachycardia (MMVT) has been shown to reduce shock frequency and improve survival. We aimed to compare cause-specific risk factors for MMVT and polymorphic ventricular tachycardia (PVT)/ventricular fibrillation (VF) and to develop predictive models.
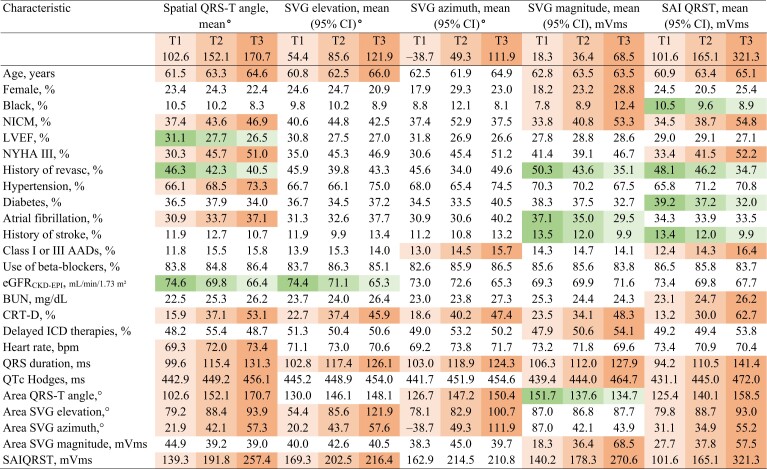
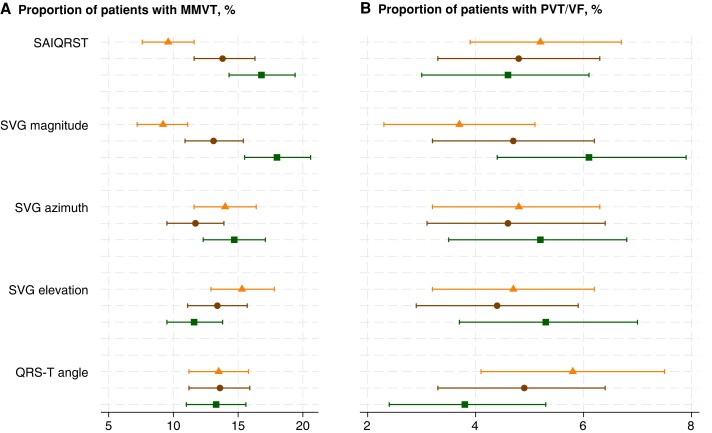
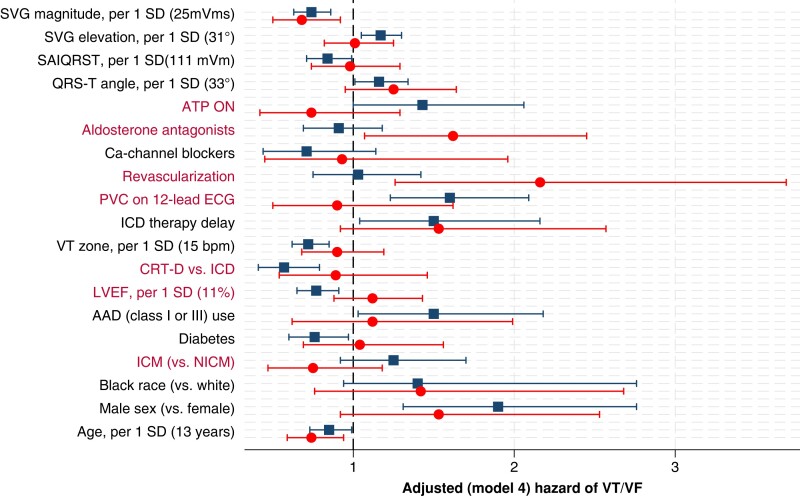
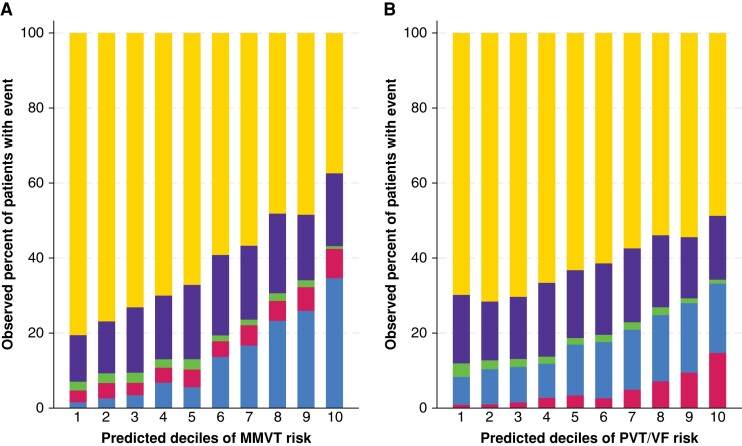
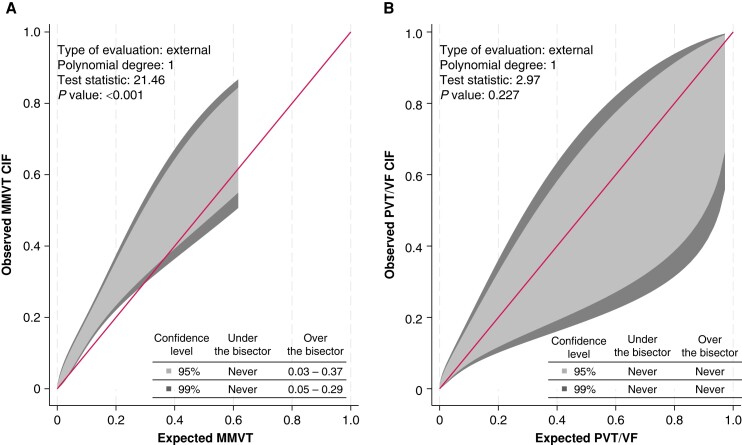
Methods and results: The multicentre retrospective cohort study included 2668 patients (age 63.1 ± 13.0 years; 23% female; 78% white; 43% non-ischaemic cardiomyopathy; left ventricular ejection fraction 28.2 ± 11.1%). Cox models were adjusted for demographic characteristics, heart failure severity and treatment, device programming, and electrocardiogram metrics. Global electrical heterogeneity was measured by spatial QRS-T angle (QRSTa), spatial ventricular gradient elevation (SVGel), azimuth, magnitude (SVGmag), and sum absolute QRST integral (SAIQRST). We compared the out-of-sample performance of the lasso and elastic net for Cox proportional hazards and the Fine-Gray competing risk model. During a median follow-up of 4 years, 359 patients experienced their first sustained MMVT with appropriate implantable cardioverter-defibrillator (ICD) therapy, and 129 patients had their first PVT/VF with appropriate ICD shock. The risk of MMVT was associated with wider QRSTa [hazard ratio (HR) 1.16; 95% confidence interval (CI) 1.01-1.34], larger SVGel (HR 1.17; 95% CI 1.05-1.30), and smaller SVGmag (HR 0.74; 95% CI 0.63-0.86) and SAIQRST (HR 0.84; 95% CI 0.71-0.99). The best-performing 3-year competing risk Fine-Gray model for MMVT [time-dependent area under the receiver operating characteristic curve (ROC(t)AUC) 0.728; 95% CI 0.668-0.788] identified high-risk (> 50%) patients with 75% sensitivity and 65% specificity, and PVT/VF prediction model had ROC(t)AUC 0.915 (95% CI 0.868-0.962), both satisfactory calibration.
Conclusion: We developed and validated models to predict the competing risks of MMVT or PVT/VF that could inform procedural planning and future randomized controlled trials of prophylactic ventricular tachycardia ablation.
Clinical trial registration: URL:www.clinicaltrials.gov Unique identifier:NCT03210883.
Keywords: HF; ICD; MMVT; PVT/VF; VCG.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: J.W.W. was on the advisory board for Heartcor Solutions for work unrelated to this publication. S.M.N. reports grant support from the National Institutes of Health (R01 HL149134 and R01 HL83359), consulting from Abbott Inc., Life Signals Inc., Uptodate Inc., and TDK Inc., intellectual property owned by the University of California Regents and Stanford University. A.J.R. reports support from the NIH (K23 HL166977) and AHA (23CDA933663). All remaining authors have declared no conflicts of interest.
Figures
Comment in
-
Electrocardiographic risk stratification in patients with a primary prophylactic implantable cardioverter defibrillator: can future arrhythmias correlating with sudden cardiac death be predicted?Europace. 2024 Jun 3;26(6):euae133. doi: 10.1093/europace/euae133. Europace. 2024. PMID: 38758091 Free PMC article.
Similar articles
-
First human safety and effectiveness study of defibrillation with a novel patch wearable cardioverter-defibrillator.Europace. 2024 Jul 2;26(7):euae189. doi: 10.1093/europace/euae189. Europace. 2024. PMID: 39001864 Free PMC article. Clinical Trial.
-
Improving sudden cardiac death risk stratification by evaluating electrocardiographic measures of global electrical heterogeneity and clinical outcomes among patients with implantable cardioverter-defibrillators: rationale and design for a retrospective, multicenter, cohort study.J Interv Card Electrophysiol. 2018 Jun;52(1):77-89. doi: 10.1007/s10840-018-0342-2. Epub 2018 Mar 14. J Interv Card Electrophysiol. 2018. PMID: 29541969 Free PMC article.
-
Performance and Safety of the Extravascular Implantable Cardioverter Defibrillator Through Long-Term Follow-Up: Final Results From the Pivotal Study.Circulation. 2025 Jan 28;151(4):322-332. doi: 10.1161/CIRCULATIONAHA.124.071795. Epub 2024 Sep 26. Circulation. 2025. PMID: 39327797 Free PMC article. Clinical Trial.
-
Impact of programming strategies aimed at reducing nonessential implantable cardioverter defibrillator therapies on mortality: a systematic review and meta-analysis.Circ Arrhythm Electrophysiol. 2014 Feb;7(1):164-70. doi: 10.1161/CIRCEP.113.001217. Epub 2014 Jan 20. Circ Arrhythm Electrophysiol. 2014. PMID: 24446023
-
A review of the evidence on the effects and costs of implantable cardioverter defibrillator therapy in different patient groups, and modelling of cost-effectiveness and cost-utility for these groups in a UK context.Health Technol Assess. 2006 Aug;10(27):iii-iv, ix-xi, 1-164. doi: 10.3310/hta10270. Health Technol Assess. 2006. PMID: 16904046
Cited by
-
Electrocardiographic risk stratification in patients with a primary prophylactic implantable cardioverter defibrillator: can future arrhythmias correlating with sudden cardiac death be predicted?Europace. 2024 Jun 3;26(6):euae133. doi: 10.1093/europace/euae133. Europace. 2024. PMID: 38758091 Free PMC article.
-
Sex differences in global electrical heterogeneity: The Hispanic Community Health Study/Study of Latinos.Heart Rhythm O2. 2024 Nov 25;6(1):97-102. doi: 10.1016/j.hroo.2024.11.019. eCollection 2025 Jan. Heart Rhythm O2. 2024. PMID: 40224258 Free PMC article. No abstract available.
-
Latent profiles of global electrical heterogeneity: the Hispanic Community Health Study/Study of Latinos.Eur Heart J Digit Health. 2024 Jul 8;5(5):611-621. doi: 10.1093/ehjdh/ztae048. eCollection 2024 Sep. Eur Heart J Digit Health. 2024. PMID: 39318685 Free PMC article.
References
-
- Fong KY, Chan YH, Wang Y, Yeo C, Lim ETS, Tan VH. Catheter ablation of ventricular arrhythmia in patients with an implantable cardioverter-defibrillator: a systematic review and meta-analysis. Can J Cardiol 2023;39:250–62. - PubMed
-
- Tung R, Xue Y, Chen M, Jiang C, Shatz DY, Besser SA et al. First-Line catheter ablation of monomorphic ventricular tachycardia in cardiomyopathy concurrent with defibrillator implantation: the PAUSE-SCD randomized trial. Circulation 2022;145:1839–49. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
