

Transanal ileal pouch-anal anastomosis: A systematic review and meta-analysis of technical approaches and clinical outcomes
- PMID: 38705912
- PMCID: PMC11070401
- DOI: 10.1007/s00423-024-03343-7
Transanal ileal pouch-anal anastomosis: A systematic review and meta-analysis of technical approaches and clinical outcomes
Abstract
Purpose: Transanal minimally invasive surgery has theoretical advantages for ileal pouch-anal anastomosis surgery. We performed a systematic review assessing technical approaches to transanal IPAA (Ta-IPAA) and meta-analysis comparing outcomes to transabdominal (abd-IPAA) approaches.
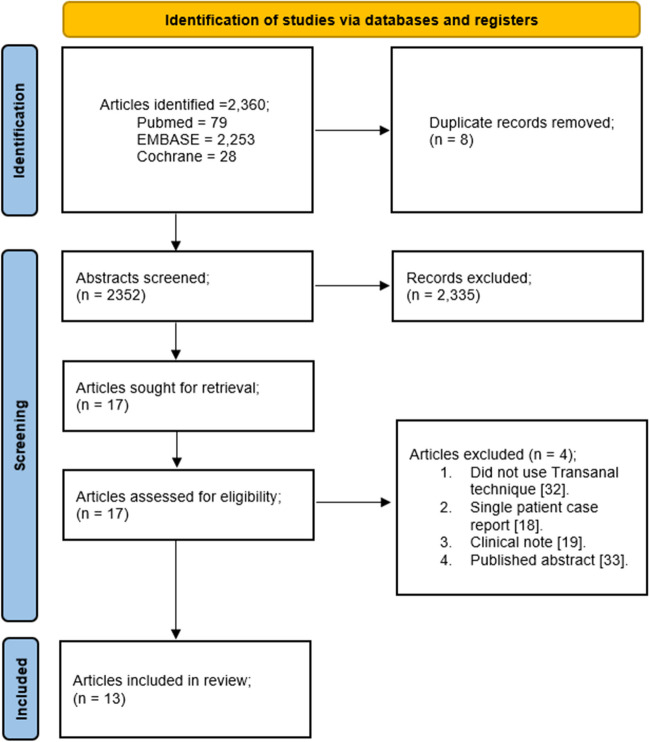
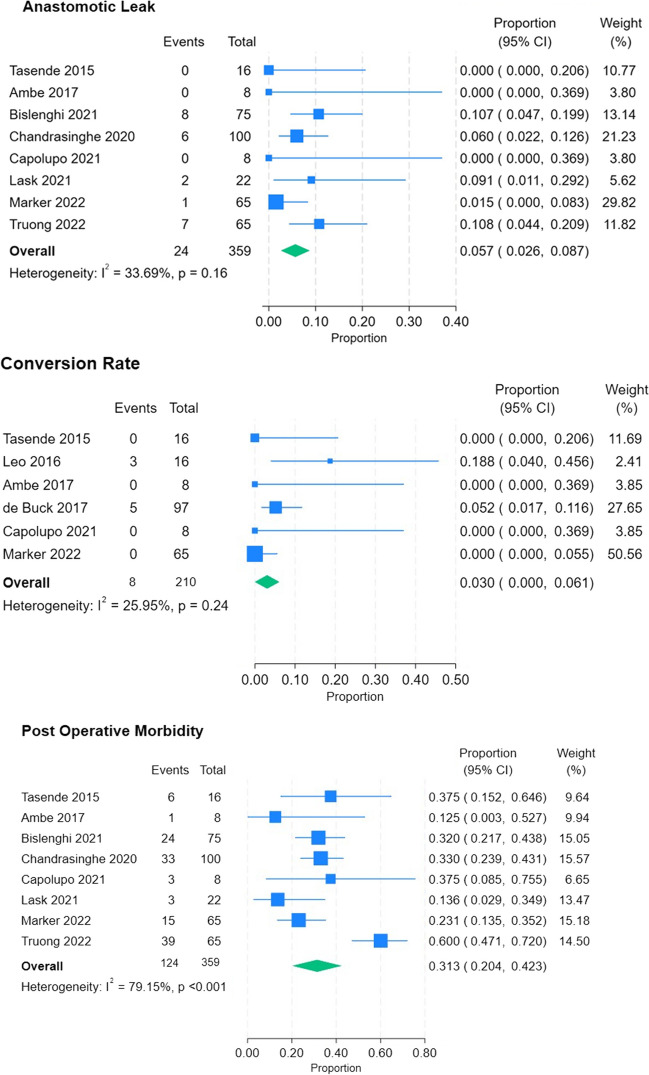
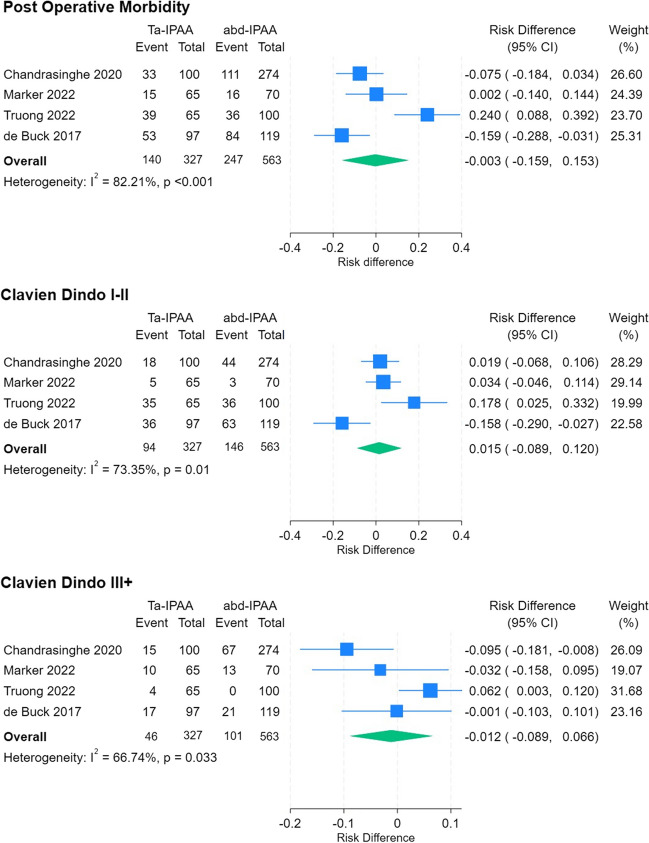
Methods: Three databases were searched for articles investigating Ta-IPAA outcomes. Primary outcome was anastomotic leak rate. Secondary outcomes included conversion rate, post operative morbidity, and length of stay (LoS). Staging, plane of dissection, anastomosis, extraction site, operative time, and functional outcomes were also assessed.
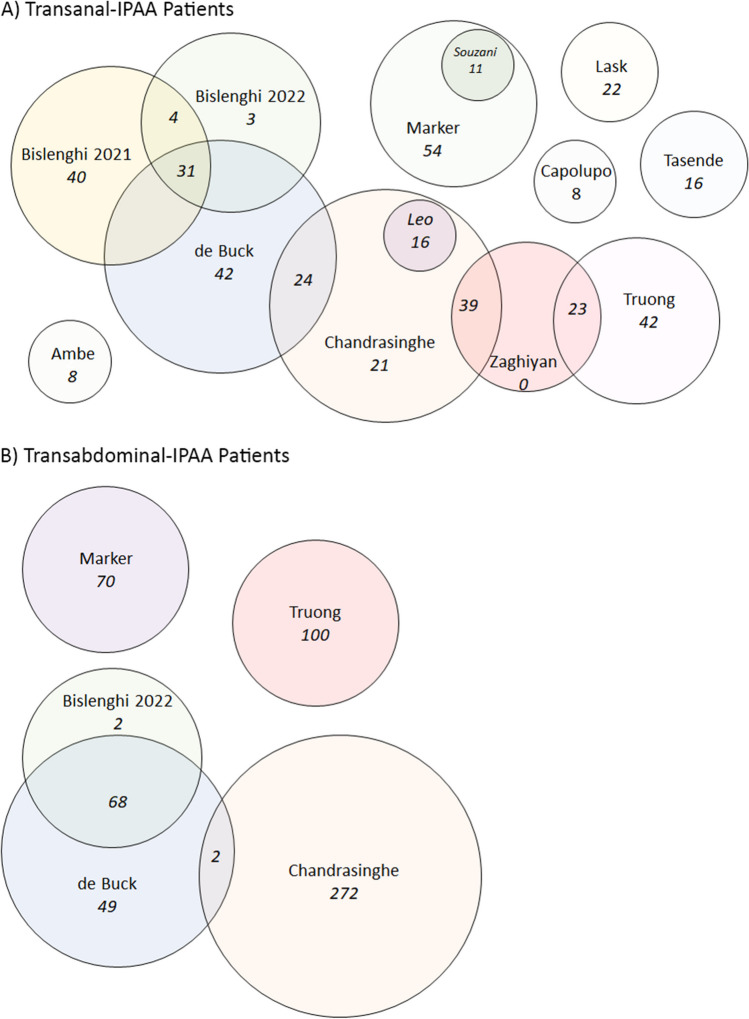
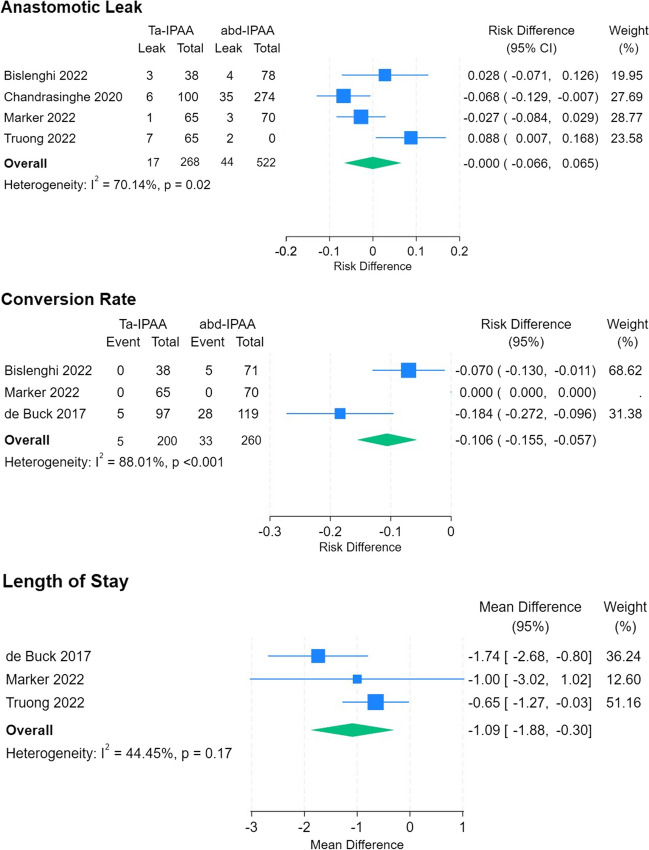
Results: Searches identified 13 studies with 404 unique Ta-IPAA and 563 abd-IPAA patients. Anastomotic leak rates were 6.3% and 8.4% (RD 0, 95% CI -0.066 to 0.065, p = 0.989) and conversion rates 2.5% and 12.5% (RD -0.106, 95% CI -0.155 to -0.057, p = 0.104) for Ta-IPAA and abd-IPAA. Average LoS was one day shorter (MD -1, 95% CI -1.876 to 0.302, p = 0.007). A three-stage approach was most common (47.6%), operative time was 261(± 60) mins, and total mesorectal excision and close rectal dissection were equally used (49.5% vs 50.5%). Functional outcomes were similar. Lack of randomised control trials, case-matched series, and significant study heterogeneity limited analysis, resulting in low to very low certainty of evidence.
Conclusions: Analysis demonstrated the feasibility and safety of Ta-IPAA with reduced LoS, trend towards less conversions, and comparable anastomotic leak rates and post operative morbidity. Though results are encouraging, they need to be interpreted with heterogeneity and selection bias in mind. Robust randomised clinical trials are warranted to adequately compare ta-IPAA to transabdominal approaches.
Keywords: Ileoanal; Meta-analysis; Systematic Review; Transanal; Ulcerative Colitis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Transanal ileal pouch-anal anastomosis for inflammatory bowel disease: a systematic review and meta-analysis of short-term outcomes.Colorectal Dis. 2024 May;26(5):886-898. doi: 10.1111/codi.16977. Epub 2024 Apr 9. Colorectal Dis. 2024. PMID: 38594838
-
A Single-Center Comparative Study of Open Transabdominal and Laparoscopic Transanal Ileal Pouch-Anal Anastomosis with Total Mesorectal Excision. Has the Bar Been Raised?J Gastrointest Surg. 2022 May;26(5):1070-1076. doi: 10.1007/s11605-021-05236-2. Epub 2022 Jan 6. J Gastrointest Surg. 2022. PMID: 34993896
-
Transanal ileal pouch anal anastomosis for ulcerative colitis in children and adults: a systematic review and meta-analysis.Pediatr Surg Int. 2022 Dec;38(12):1671-1680. doi: 10.1007/s00383-022-05222-y. Epub 2022 Sep 17. Pediatr Surg Int. 2022. PMID: 36114863
-
Transanal Ileal Pouch-Anal Anastomosis for Ulcerative Colitis has Comparable Long-Term Functional Outcomes to Transabdominal Approach: A Multicentre Comparative Study.J Crohns Colitis. 2020 Jul 9;14(6):726-733. doi: 10.1093/ecco-jcc/jjz174. J Crohns Colitis. 2020. PMID: 31637417
-
Transanal ileal pouch-anal anastomosis for ulcerative colitis: a single-center comparative study.Tech Coloproctol. 2022 Nov;26(11):875-881. doi: 10.1007/s10151-022-02658-1. Epub 2022 Aug 10. Tech Coloproctol. 2022. PMID: 35947241
Cited by
-
[An update on surgical treatment options for inflammatory bowel disease].Inn Med (Heidelb). 2025 Feb;66(2):174-180. doi: 10.1007/s00108-024-01846-5. Epub 2025 Jan 30. Inn Med (Heidelb). 2025. PMID: 39883175 Free PMC article. Review. German.
References
-
- Aquina C, Fleming F, Becerra A, et al. Who gets a pouch after colectomy in New York state and why? Dis Colon Rectum. 2016;59:e109–e110. doi: 10.1097/01.dcr.0000482708.50838.af. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
