

Effects of the COVID-19 pandemic on short-term postoperative outcomes for colorectal perforation: A nationwide study in Japan based on the National Clinical Database
- PMID: 38707225
- PMCID: PMC11066486
- DOI: 10.1002/ags3.12758
Effects of the COVID-19 pandemic on short-term postoperative outcomes for colorectal perforation: A nationwide study in Japan based on the National Clinical Database
Abstract
Aim: Possible negative effects of the COVID-19 pandemic on short-term postoperative outcomes for colorectal perforation in Japan were examined in this study.
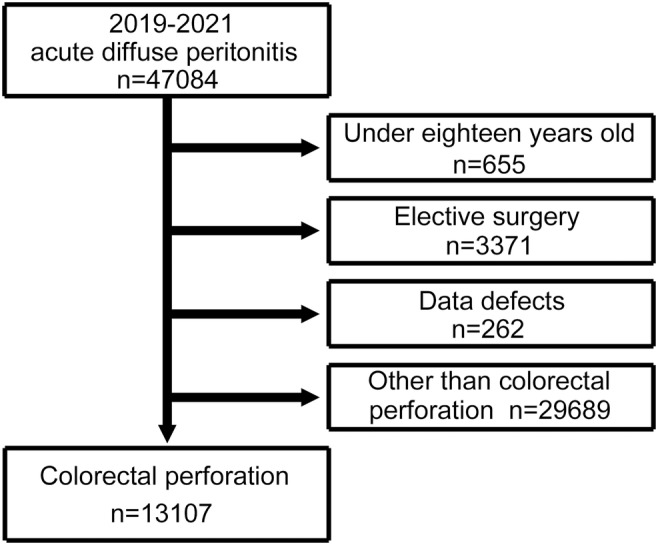
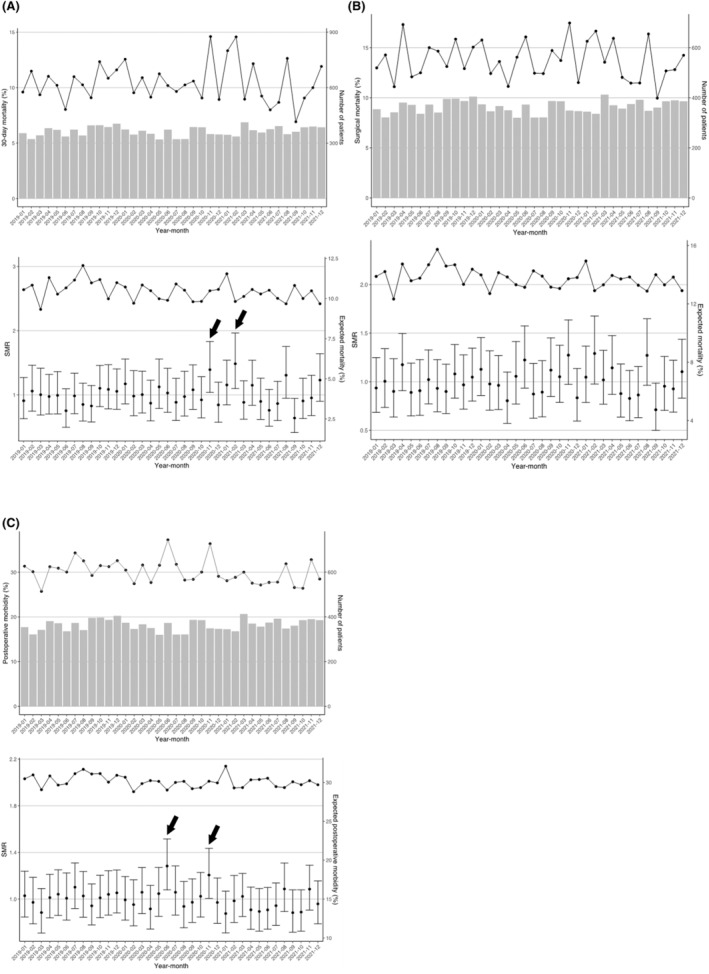
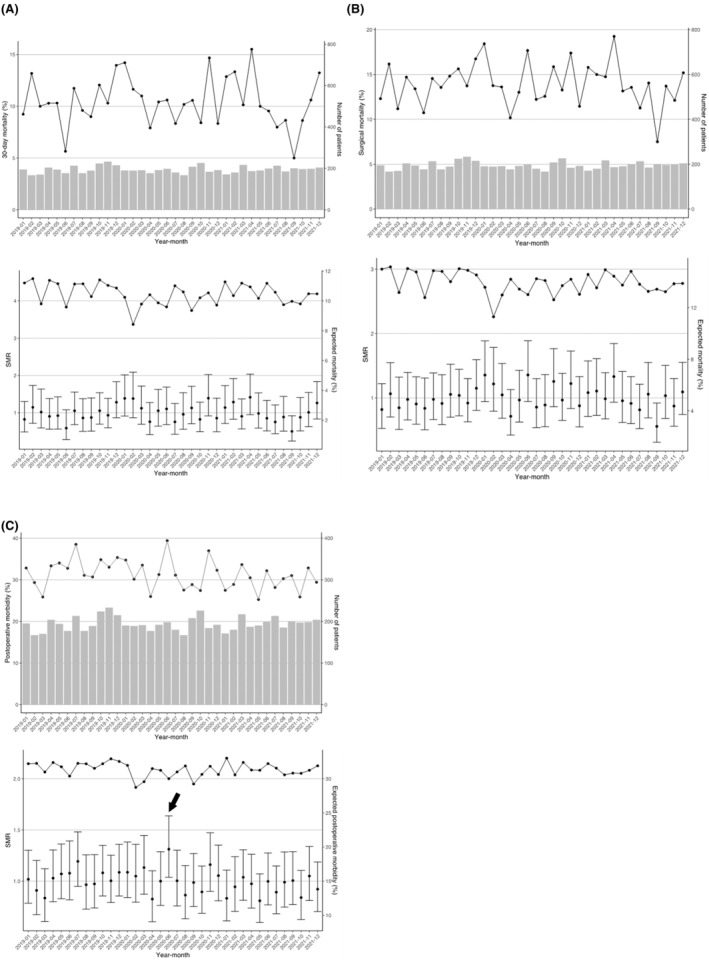
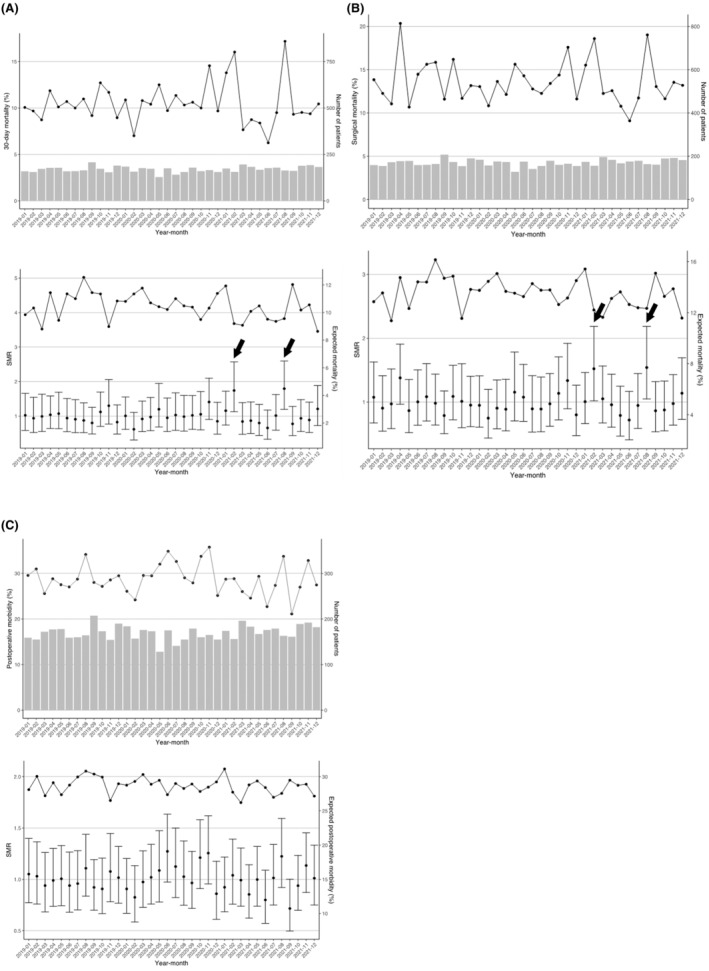
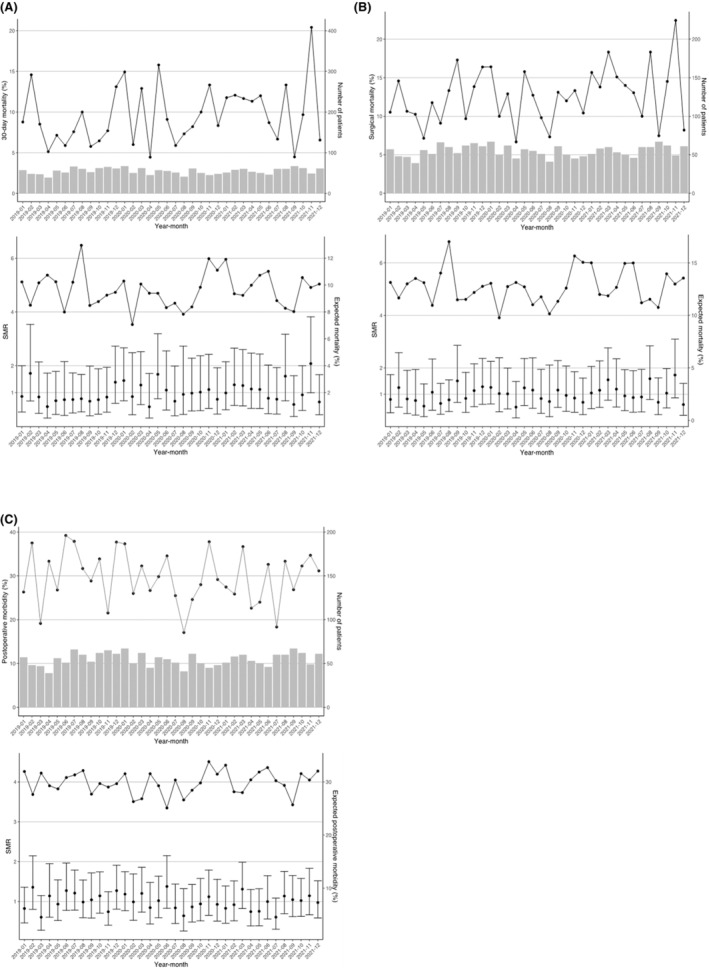
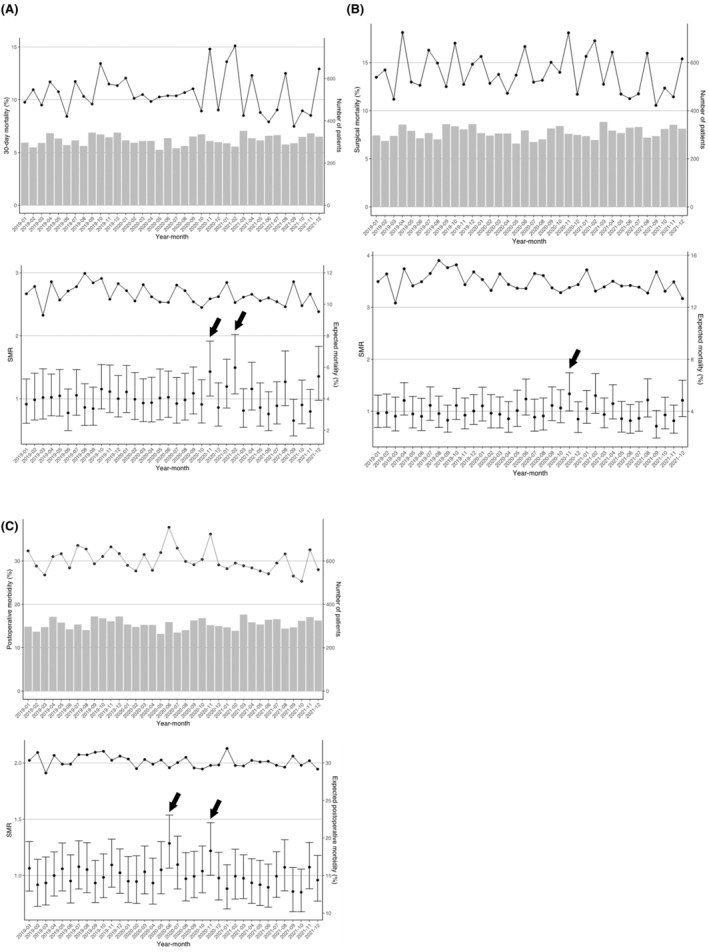
Methods: The National Clinical Database (NCD) is a large-scale database including more than 95% of surgical cases in Japan. We analyzed 13 107 cases of colorectal perforation from 2019 to 2021. National data were analyzed, and subgroup analyses were conducted for subjects in prefectures with high infection levels (HILs) and metropolitan areas (Tokyo Met. and Osaka Pref.). Postoperative 30-day mortality, surgical mortality, and postoperative complications (Clavien-Dindo grade ≥3) were examined. Months were considered to have significantly high or low mortality or complication rates, if the 95% confidence interval (CI) of the standardized mortality (morbidity) ratio (SMR) does not contain 1.
Results: In the NCD, postoperative 30-day mortality occurred in 1371 subjects (10.5%), surgical mortality in 1805 (13.8%), and postoperative complications in 3950 (30.1%). Significantly higher SMRs were found for 30-day mortality in November 2020 (14.6%, 1.39 [95% CI: 1.04-1.83]) and February 2021 (14.6%, 1.48 [95% CI: 1.10-1.96]), and for postoperative complications in June 2020 (37.3%, 1.28 [95% CI: 1.08-1.52]) and November 2020 (36.4%, 1.21 [95% CI: 1.01-1.44]). The SMRs for surgical mortality were not significantly high in any month. In prefectures with HILs and large metropolitan areas, there were few months with significantly higher SMRs.
Conclusions: The COVID-19 pandemic had limited negative effects on postoperative outcomes in patients with colorectal perforation. These findings suggest that the emergency system for colorectal perforation in Japan was generally maintained during the pandemic.
Keywords: COVID‐19; National Clinical Database; colorectal perforation; postoperative short‐term outcomes.
© 2023 The Authors. Annals of Gastroenterological Surgery published by John Wiley & Sons Australia, Ltd on behalf of The Japanese Society of Gastroenterological Surgery.
Conflict of interest statement
Hideki Endo and Hiroyuki Yamamoto are affiliated with the Department of Healthcare Quality Assessment at the University of Tokyo. The department is a social collaboration department supported by grants from the National Clinical Database, Intuitive Surgical Sarl, Johnson & Johnson K.K., and Nipro Co. Yuko Kitagawa is Editor‐in‐Chief of Annals of Gastroenterological Surgery. Masaki Mori is Emeritus Editor‐in‐Chief of Annals of Gastroenterological Surgery. Yoshihiro Kakeji and Hideki Ueno are Associate Editors of Annals of Gastroenterological Surgery dealing with the lower digestive tract. The other authors declare no conflicts of interest for this article.
Figures
Similar articles
-
Effects of the COVID-19 pandemic on short-term postoperative outcomes of emergency surgery for gastroduodenal perforation: A nationwide study in Japan based on the National Clinical Database.Ann Gastroenterol Surg. 2024 Apr 15;8(5):795-806. doi: 10.1002/ags3.12806. eCollection 2024 Sep. Ann Gastroenterol Surg. 2024. PMID: 39229559 Free PMC article.
-
Effects of an increase in emergency cases with difficulties in transport to hospital during the COVID-19 pandemic on postoperative short-term outcomes of colorectal perforation: A study based on the National Clinical Database.Ann Gastroenterol Surg. 2024 Nov 27;9(3):505-517. doi: 10.1002/ags3.12887. eCollection 2025 May. Ann Gastroenterol Surg. 2024. PMID: 40385336 Free PMC article.
-
Impact of the COVID-19 pandemic on short-term outcomes after pancreaticoduodenectomy for pancreatic cancer: A retrospective study from the Japanese National Clinical Database, 2018-2021.Ann Gastroenterol Surg. 2024 Mar 23;8(5):877-887. doi: 10.1002/ags3.12798. eCollection 2024 Sep. Ann Gastroenterol Surg. 2024. PMID: 39229557 Free PMC article.
-
IMPACT OF THE COVID-19 PANDEMIC ON THE EMERGENCY SURGICAL TREATMENT OF COLORECTAL CANCER.Arq Bras Cir Dig. 2024 Feb 5;36:e1793. doi: 10.1590/0102-672020230075e1793. eCollection 2024. Arq Bras Cir Dig. 2024. PMID: 38324854 Free PMC article. Review.
-
Local versus radical surgery for early rectal cancer with or without neoadjuvant or adjuvant therapy.Cochrane Database Syst Rev. 2023 Jun 13;6(6):CD002198. doi: 10.1002/14651858.CD002198.pub3. Cochrane Database Syst Rev. 2023. PMID: 37310167 Free PMC article. Review.
Cited by
-
Effects of the COVID-19 pandemic on short-term postoperative outcomes of emergency surgery for gastroduodenal perforation: A nationwide study in Japan based on the National Clinical Database.Ann Gastroenterol Surg. 2024 Apr 15;8(5):795-806. doi: 10.1002/ags3.12806. eCollection 2024 Sep. Ann Gastroenterol Surg. 2024. PMID: 39229559 Free PMC article.
-
Effects of an increase in emergency cases with difficulties in transport to hospital during the COVID-19 pandemic on postoperative short-term outcomes of colorectal perforation: A study based on the National Clinical Database.Ann Gastroenterol Surg. 2024 Nov 27;9(3):505-517. doi: 10.1002/ags3.12887. eCollection 2025 May. Ann Gastroenterol Surg. 2024. PMID: 40385336 Free PMC article.
-
Impacts of COVID-19 pandemic on short-term outcomes of low anterior resection performed in hospitals with different surgical volumes.Ann Gastroenterol Surg. 2024 Dec 23;9(3):608-618. doi: 10.1002/ags3.12900. eCollection 2025 May. Ann Gastroenterol Surg. 2024. PMID: 40385348 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
