

Review
doi: 10.1097/CLD.0000000000000158.
eCollection 2024 Jan-Jun.
Approach to immunotherapy for HCC in the liver transplant population
Affiliations
- PMID: 38707244
- PMCID: PMC11068135
- DOI: 10.1097/CLD.0000000000000158
Item in Clipboard
Review
Approach to immunotherapy for HCC in the liver transplant population
Clin Liver Dis (Hoboken).
.
No abstract available
Conflict of interest statement
Mario Strazzabosco consults for Engitix. The remaining authors have no conflicts to report.
Figures

Mechanistic rationale for neoadjuvant and adjuvant immunotherapy in HCC treatment. In A, the immunomodulatory effects of the 3 major classes of immunotherapies utilized for HCC treatment are summarized. Immune checkpoint inhibitors include anti-PD-1 (eg, nivolumab, pembrolizumab), anti-PDL-1 (eg, atezolizumab, durvalumab), and anti-CTLA-4 agents. (eg, ipilimumab). Antibodies designed to inhibit immune checkpoint receptor-ligand interactions (eg PD-1/PDL-1 and CTLA-4/CD80) restore T cell activation within the tumor microenvironment, enhancing immune-mediated anti-tumor responses. VEGF inhibitors (eg, bevacizumab) affect angiogenesis within the tumor microenvironment, leading to relative tumor hypoxia (vessel pruning) and may also improve drug delivery and mobilization of immune cells by normalization of the tumoral vasculature. In B, the rationale for immunotherapy as adjuvant or neoadjuvant therapy is graphically depicted. Immunotherapy before surgery or LRT (termed neoadjuvant use) augments immune-mediated anti-tumor response, potentially reducing tumor burden and treating microscopic (eg, nonvisible) disease. This could improve outcomes of definitive therapeutic interventions by reducing the size of the tumor before resection or ablation and may ultimately reduce rates of postoperative tumor recurrence. A concern with neoadjuvant therapy is that it may delay the time to definitive therapeutic interventions. Immunotherapy after curative interventions (term adjuvant use) has demonstrated clinical benefit in reducing HCC recurrence in cases of tumors with high-risk features. Surgical resection or LRT induces cell necrosis and release of tumor antigens, which is thought to favorably alter the tumor microenvironment and enhance the immune-mediated effects of immunotherapy. Abbreviations: Anti-CTLA-4, anti-cytotoxic T lymphocyte–associated protein-4; Anti-PDL-1, anti-programmed cell death ligand-1; APC, antigen-presenting cell; CTLA-4 (cytotoxic T lymphocyte-associated protein-4); DC, dendritic cell; LRT, locoregional therapy; PD-1, programmed cell death-1; PDL-1, programmed cell death ligand-1; TAM, tumor-associated macrophage; TME, tumor microenvironment.
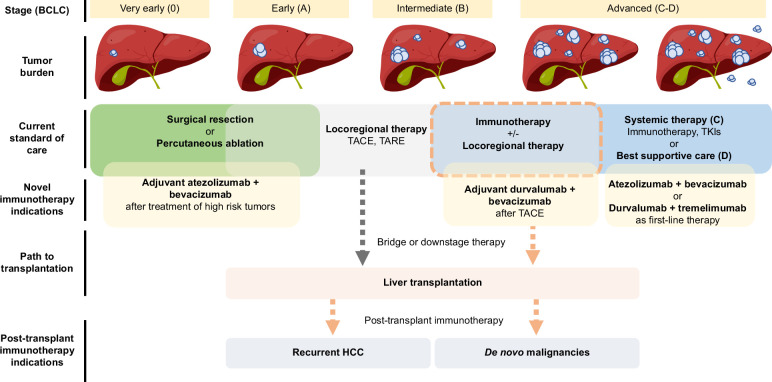
Evolving treatment paradigm for HCC. This figure summarizes the general treatment approach to HCC based on the stage of disease, highlighting expanding indications for immunotherapy across all stages of disease. Novel indications for immunotherapy with established efficacy are outlined in the figure, including use of adjuvant atezolizumab and bevacizumab after treatment of early-stage tumors with high-risk features (IMBravo050 trial), adjuvant durvalumab and bevacizumab after TACE for unresectable tumors (EMERALD-1 trial), and first-line use of either atezolizumab and bevacizumab or durvalumab and tremelimumab for unresectable advanced stages of HCC (IMBrave150 and HIMALAYA trials, respectively). Though standalone regimens with locoregional therapy are the current standard approach to bridging or downstaging therapy before liver transplantation (gray dotted arrow), there may be a role for immunotherapeutic regimens as bridging or downstaging treatments before liver transplantation for both intermediate and advanced stages of HCC (orange dotted lines). Treatment of recurrent HCC or de novo nonhepatic malignancies in the posttransplant setting with immunotherapies is also a viable area. Liver image licensed through iStock Getty Images (stock file ID: 1295846316). Abbreviations: BCLC, Barcelona Clinic Liver Cancer; TACE, transarterial chemoembolization; TARE, transarterial radioembolization; TKIs, tyrosine kinase inhibitors.

Rationale and risk of immunotherapy peri-liver transplantation. Immunotherapy for HCC before liver transplantation is used as downstaging or bridging therapy. Its use in the posttransplant setting includes treatment of recurrent HCC or de novo nonhepatic malignancy. In either circumstance, immunotherapy pretransplantation or posttransplantation poses a risk of allograft liver rejection. Expression of immune checkpoint inhibitor ligands (eg, PDL-1) may potentiate the risk of allograft rejection. Abbreviations: anti-PD-1, anti-programmed cell death-1; anti-PDL-1, anti-programmed cell death ligand-1.
References
-
- Finn RS, Qin S, Ikeda M, Galle PR, Ducreux M, Kim TY, et al. . Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382:1894–1905. - PubMed
-
- Abou-Alfa GK, Lau G, Kudo M, Chan SL, Kelley RK, Furuse J, et al. . Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid. 2022;1:EVIDoa2100070. - PubMed
-
- Qin S, Chen M, Cheng AL, Kaseb AO, Kudo M, Lee HC, et al. . Atezolizumab plus bevacizumab versus active surveillance in patients with resected or ablated high-risk hepatocellular carcinoma (IMbrave050): A randomised, open-label, multicentre, phase 3 trial. Lancet. 2023;402:1835–1847. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
