

Prediction of small intracranial aneurysm rupture status based on combined Clinical-Radiomics model
- PMID: 38707310
- PMCID: PMC11066671
- DOI: 10.1016/j.heliyon.2024.e30214
Prediction of small intracranial aneurysm rupture status based on combined Clinical-Radiomics model
Abstract
Background: Accumulating small unruptured intracranial aneurysms are detected due to the improved quality and higher frequency of cranial imaging, but treatment remains controversial. While surgery or endovascular treatment is effective for small aneurysms with a high risk of rupture, such interventions are unnecessary for aneurysms with a low risk of rupture. Consequently, it is imperative to accurately identify small aneurysms with a low risk of rupture. The purpose of this study was to develop a clinically practical model to predict small aneurysm ruptures based on a radiomics signature and clinical risk factors.
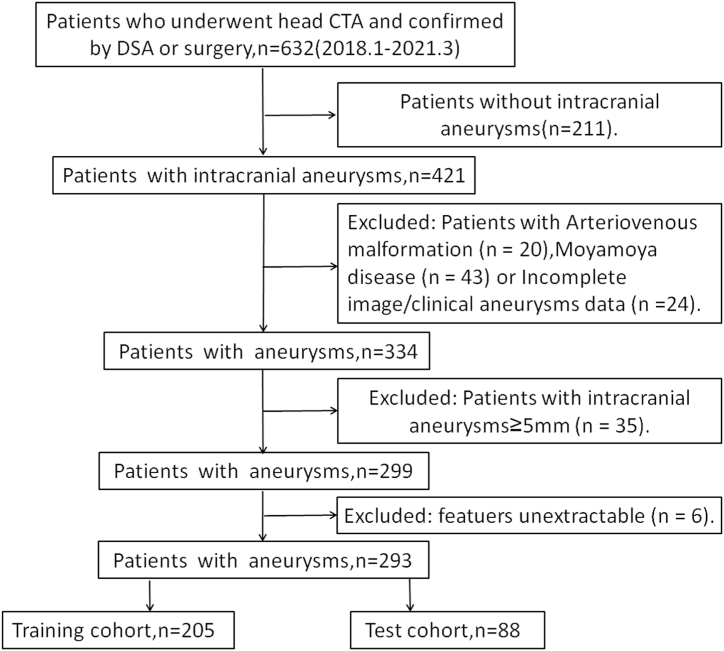
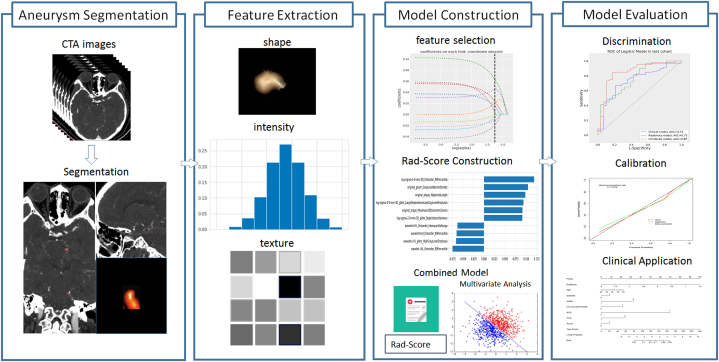
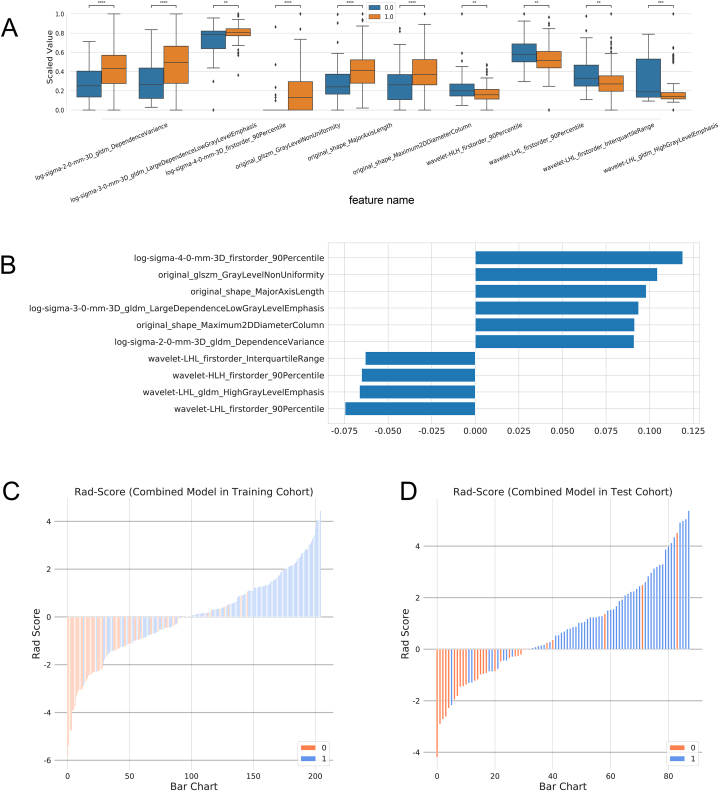
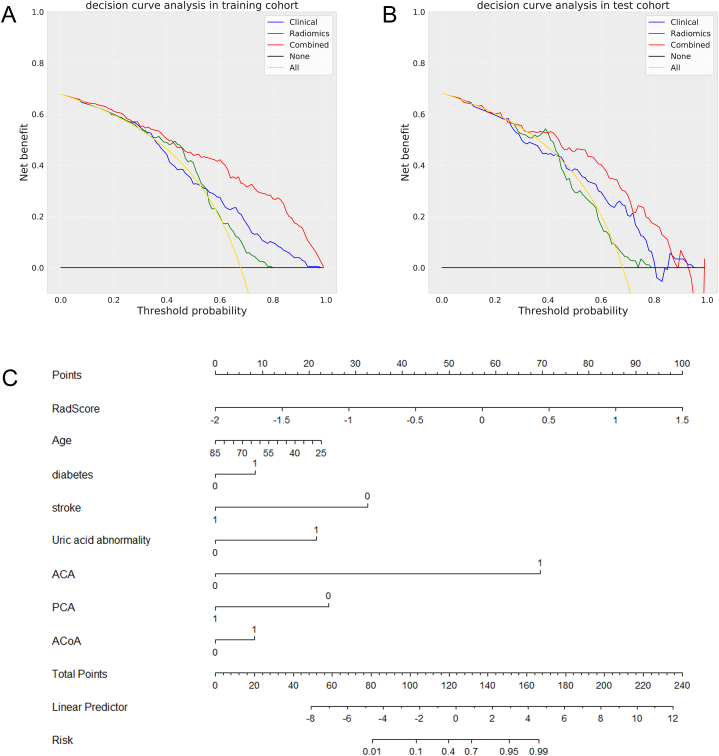
Methods: A total of 293 patients having an aneurysm with a diameter of less than 5 mm, including 199 patients (67.9 %) with a ruptured aneurysm and 94 patients (32.1 %) without a ruptured aneurysm, were included in this study. Digital subtraction angiography or surgical treatment was required in all cases. Data on the clinical risk factors and the features on computed tomography angiography images associated with the aneurysm rupture status were collected simultaneously. We developed a clinical-radiomics model to predict aneurysm rupture status using multivariate logistic regression analysis. The combined clinical-radiomics model was constructed by nomogram analysis. The diagnostic performance, clinical utility, and model calibration were evaluated by operating characteristic curve analysis, decision curve analysis, and calibration analysis.
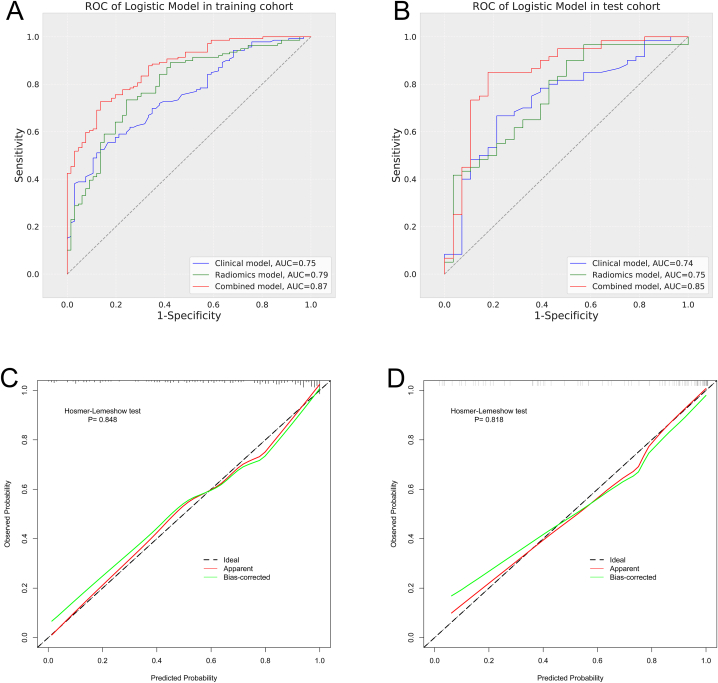
Results: A combined clinical-radiomics model (Area Under Curve [AUC], 0.85; 95 % confidence interval [CI], 0.757-0.947) showed effective performance in the operating characteristic curve analysis. In the validation cohort, the performance of the combined model was better than that of the radiomics model (AUC, 0.75; 95 % CI, 0.645-0.865; Delong's test p-value = 0.01) and the clinical model (AUC, 0.74; 95 % CI, 0.625-0.851; Delong's test p-value <0.01) alone. The results of the decision curve, nomogram, and calibration analyses demonstrated the clinical utility and good fitness of the combined model.
Conclusion: Our study demonstrated the effectiveness of a clinical-radiomics model for predicting rupture status in small aneurysms.
© 2024 The Authors. Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Clinical-Radiomics Nomogram Model Based on CT Angiography for Prediction of Intracranial Aneurysm Rupture: A Multicenter Study.J Multidiscip Healthc. 2024 Dec 10;17:5917-5926. doi: 10.2147/JMDH.S491697. eCollection 2024. J Multidiscip Healthc. 2024. PMID: 39678712 Free PMC article.
-
A preliminary investigation of radiomics differences between ruptured and unruptured intracranial aneurysms.Eur Radiol. 2021 May;31(5):2716-2725. doi: 10.1007/s00330-020-07325-3. Epub 2020 Oct 14. Eur Radiol. 2021. PMID: 33052466
-
Development and validation of a deep learning model for prediction of intracranial aneurysm rupture risk based on multi-omics factor.Eur Radiol. 2023 Oct;33(10):6759-6770. doi: 10.1007/s00330-023-09672-3. Epub 2023 Apr 26. Eur Radiol. 2023. PMID: 37099175
-
Accuracy of radiomics-Based models in distinguishing between ruptured and unruptured intracranial aneurysms: A systematic review and meta-Analysis.Eur J Radiol. 2024 Dec;181:111739. doi: 10.1016/j.ejrad.2024.111739. Epub 2024 Sep 16. Eur J Radiol. 2024. PMID: 39293240
-
Predictive value of radiomics for intracranial aneurysm rupture: a systematic review and meta-analysis.Front Neurosci. 2024 Oct 9;18:1474780. doi: 10.3389/fnins.2024.1474780. eCollection 2024. Front Neurosci. 2024. PMID: 39445076 Free PMC article.
Cited by
-
Two possible hemodynamic mechanisms underlying the growth of cerebral aneurysms depending on their size: The NHO CFD ABO study.J Cereb Blood Flow Metab. 2025 Mar 13:271678X251325972. doi: 10.1177/0271678X251325972. Online ahead of print. J Cereb Blood Flow Metab. 2025. PMID: 40079558 Free PMC article.
-
Systematic Review of Radiomics and Artificial Intelligence in Intracranial Aneurysm Management.J Neuroimaging. 2025 Mar-Apr;35(2):e70037. doi: 10.1111/jon.70037. J Neuroimaging. 2025. PMID: 40095247 Free PMC article.
-
Diagnostic and predictive value of radiomics-based machine learning for intracranial aneurysm rupture status: a systematic review and meta-analysis.Neurosurg Rev. 2024 Nov 12;47(1):845. doi: 10.1007/s10143-024-03086-5. Neurosurg Rev. 2024. PMID: 39528874 Free PMC article.
References
-
- Claassen J., Park S. Spontaneous subarachnoid haemorrhage. Lancet. 2022;400(10355):846–862. https://doi:10.1016/S0140-6736(22)00938-2 - DOI - PMC - PubMed
-
- Jin H., Geng J., Yin Y., et al. Fully automated intracranial aneurysm detection and segmentation from digital subtraction angiography series using an end-to-end spatiotemporal deep neural network. J. Neurointerventional Surg. 2020;12(10):1023–1027. https://doi:10.1136/neurintsurg-2020-015824 - DOI - PubMed
-
- Varble N., Tutino V.M., Yu J., et al. Shared and distinct rupture discriminants of small and large intracranial aneurysms. Stroke. 2018;49(4):856–864. https://doi:10.1161/STROKEAHA.117.0199294 - DOI - PMC - PubMed
-
- Backes D., Rinkel G.J., Laban K.G., Algra A., Vergouwen M.D. Patient- and aneurysm-specific risk factors for intracranial aneurysm growth: a systematic review and meta-analysis. Stroke. 2016;47(4):951–957. https://doi:10.1161/STROKEAHA.115.0121625 - DOI - PubMed
-
- Brown RD Jr, Broderick J.P. Unruptured intracranial aneurysms: epidemiology, natural history, management options, and familial screening. Lancet Neurol. 2014;13(4):393–404. https://doi:10.1016/S1474-4422(14)70015-8 - DOI - PubMed
LinkOut - more resources
Full Text Sources
