

Novel all-arthroscopic biceps tenodesis technique incorporated into rotator cuff repair-two hundred cases with minimum 2-year follow-up
- PMID: 38707557
- PMCID: PMC11064578
- DOI: 10.1016/j.jseint.2023.07.008
Novel all-arthroscopic biceps tenodesis technique incorporated into rotator cuff repair-two hundred cases with minimum 2-year follow-up
Abstract
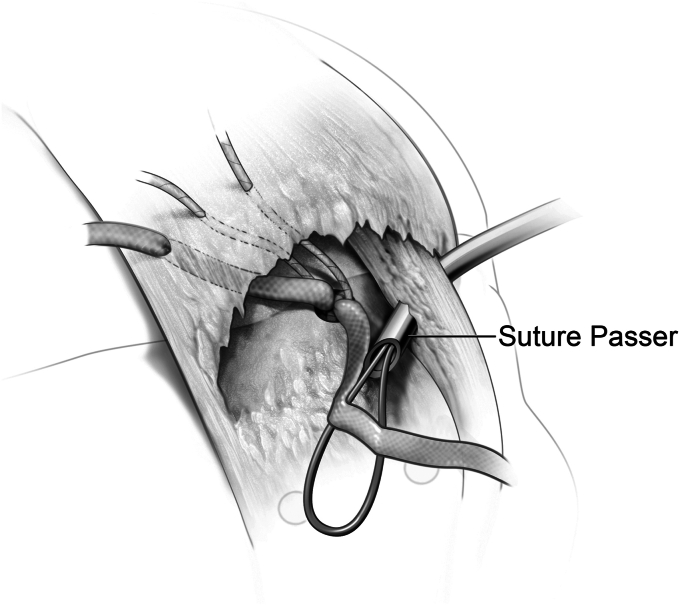
Background: Biceps tendon pathology is a common source of pain in the shoulder. It is frequently seen in conjunction with symptomatic rotator cuff tears. Biceps tendon management during arthroscopic rotator cuff repairs can be achieved via tenodesis with various techniques or tenotomy. Tenodesis of the biceps generally results in less deformity and reduced exertion-related cramping. However, most techniques require the addition of some type of hardware to provide fixation for the biceps tendon, which adds cost, time, and complexity. This study presents a technique for an all-arthroscopic bicep tenodesis performed in conjunction with a double-row rotator cuff repair, requiring no additional hardware.
Methods: This study is a retrospective review of data that were prospectively collected for 200 consecutive patients for whom the procedure was performed. Patients were seen postoperatively at 2 weeks, 6 weeks, 4 months, and 6 months and in addition massive rotator cuff repairs were seen at 8 months. Additionally all patients were contacted at a minimum 2-year follow-up to access for the presence deformity, the American Shoulder and Elbow Surgeons (ASES) score, and SANE score. Descriptive statistics and comparisons to known minimal clinical important differences (MCIDs) for the patient recorded outcome measures were recorded.
Results: Two hundred patients were included in the study and 152 responded to the telephone interviews. The mean age of the patients at the time of surgery was 65.3 year old (standard deviation ± 9.1, range of 46-84), and the mean postoperative phone interview was 3.2 years postsurgery (standard deviation of ± 1.0, range of 2-5 years). The average ASES score improved from 52.6 to 94.6, which is 3 times greater than the minimal clinical important difference. The average postoperative SANE score was 94. Seven procedures out of the 200 were labeled as failures due to 1 patient's nonsatisfaction with the procedure and 3 for a Popeye deformity and 3 that had a revision RCR.
Discussion: The described method of an arthroscopic biceps tenodesis performed with a rotator cuff repair uses no extra hardware, requires minimal additional operative time, and is clinically effective. At a minimum 2-year follow-up, the all-arthroscopic biceps tenodesis in conjunction with a double-row rotator cuff repair resulted in a marked improvement in their ASES score with a 3.5% failure rate.
Conclusion: The all-arthroscopic bicep tenodesis performed in conjunction with a double-row rotator cuff repair demonstrated improved clinical outcome, without requiring any additional hardware to tenodese the biceps, at a minimum 2-year follow-up.
Keywords: Arthroscopic; Bicep tendon; Bicep tenodesis; Double row; Rotator cuff; Rotator cuff tear.
© 2023 The Authors.
Figures






References
LinkOut - more resources
Full Text Sources