

Outcomes following duodenectomy in patients with familial adenomatous polyposis
- PMID: 38707599
- PMCID: PMC11068438
- DOI: 10.1055/a-2298-0038
Outcomes following duodenectomy in patients with familial adenomatous polyposis
Abstract
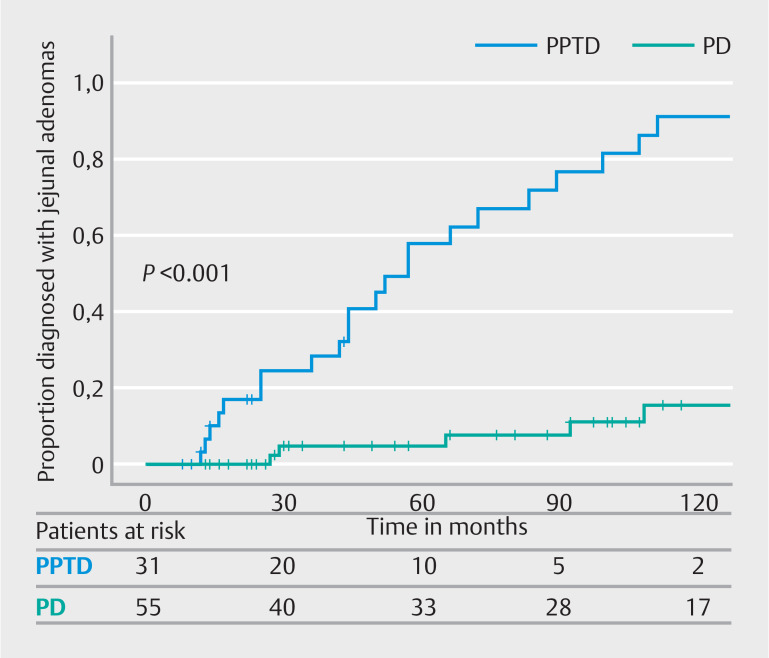
Background and study aims Some patients with familial adenomatous polyposis (FAP) and extensive duodenal polyposis or cancer require total duodenectomy. Regular postoperative endoscopic surveillance of the remaining jejunum and stomach is recommended, but little is known about the outcomes after this surgery. Patients and methods Patients with FAP who underwent either pancreatoduodenectomy (PD) or pancreas-preserving total duodenectomy (PPTD) were identified at two expert centers. Data about postoperative endoscopic surveillance outcomes were collected, as well as survival outcomes. Results Overall, 119 patients (50% female) underwent duodenectomy (86 PD and 33 PPTD); 100 for benign duodenal polyposis and 19 for duodenal or ampullary cancer. Details of postoperative endoscopic surveillance were available for 88 patients (74%). During a median follow-up of 106 months, 36 patients (41%) were diagnosed with jejunal adenomas after duodenectomy, with a significantly higher proportion in patients who underwent PPTD compared with patients who underwent PD (log-rank, P < 0.01). Two patients developed jejunal cancer (2%). Twenty-six patients (30%) were diagnosed with a total of 66 gastric adenomas, of which 61% were located in the fundus/body and 39% in the antrum. Five patients (6%) developed gastric cancer after a median of 15 years (range 6-23 years), all but one within carpeting fundic gland polyposis. Patients who underwent surgery for cancer had worse survival than patients with benign disease and all but one patient with postoperative gastric/jejunal cancer died. Conclusions After duodenectomy in FAP, a considerable risk of developing adenomas and cancer in the stomach and jejunum exists with poor cancer prognosis, highlighting the need for close postoperative endoscopic surveillance.
Keywords: Familial adenomatous polyposis; duodenal surgery; endoscopic surveillance; gastric neoplasia; jejunal neoplasia.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
Conflict of Interest Arthur S. Aelvoet: none to declare. Isabel Martin: none to declare. James Cockburn: none to declare. Cherryl Cabalit: none to declare. Victoria Cuthill: none to declare. Duncan Spalding: none to declare. Olivier R. Busch: none to declare. Barbara A.J. Bastiaansen: speakers' fee from Olympus, Tillotts Pharma AG and Ovesco Endoscopy AG. Susan K. Clark: none to declare. Evelien Dekker: endoscopic equipment on loan of FujiFilm and Olympus, research grant from FujiFilm, consultancy for FujiFilm, Olympus, Ambu and InterVenn, and speakers' fee from Olympus, GI Supply, Norgine, IPSEN, PAION and FujiFilm. Andrew Latchford: none to declare.
Figures


References
-
- Anele CC, Xiang J, Martin I et al. Regular endoscopic surveillance and polypectomy is effective in managing rectal adenoma progression following colectomy and ileorectal anastomosis in patients with familial adenomatous polyposis. Colorectal Dis. 2022;24:277–283. - PubMed
-
- Ghorbanoghli Z, Bastiaansen BA, Langers AM et al. Extracolonic cancer risk in Dutch patients with APC (adenomatous polyposis coli)-associated polyposis. J Med Genetics. 2018;55:11–14. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous