

Modification of an Airway Training Mannequin to Teach Engagement of the Hyoepiglottic Ligament
- PMID: 38707943
- PMCID: PMC11068319
- DOI: 10.21980/J8R06P
Modification of an Airway Training Mannequin to Teach Engagement of the Hyoepiglottic Ligament
Abstract
Audience: This airway trainer modification is designed to instruct all levels of training in emergency medicine in order to familiarize trainees with airway anatomy and obtain superior views of the glottic inlet.
Introduction: During intubation with a standard geometry laryngoscope, such as the Macintosh blade, placement of the distal end of the blade within the vallecula and engagement of the median glossoepiglottic fold, also referred to as the midline vallecular fold (MVF), has long been championed by experts in airway management for its ability to improve glottic inlet visualization. This notion was further supported by the recent publication of a retrospective video review by Driver et al.1 Unfortunately, airway anatomy, including engagement of the MVF, does not receive the emphasis it deserves during intubation training of emergency medicine residents. Emergency physicians often have limited time to perform complete airway examinations, but a sound recognition and appreciation of the laryngeal inlet can serve as a roadmap to optimal laryngoscopy.2Recent advancements in airway education emphasize visualization of airway anatomy with review of video laryngoscopy (VL) recordings to identify routine VL errors in vallecula manipulation, such as failure to engage the MVF. 3 Simulation can continue to play an essential role in enhancing trainees' airway skills. Current airway trainers lack functional fidelity components, such an engageable MVF, resulting in a missed opportunity to teach airway skills and anatomy in a safe and controlled setting.4, 5 To address these concerns, we modified an existing airway task trainer with the addition of a simulated MVF to expose trainees to airway anatomy and adequate MVF engagement resulting in epiglottic elevation.
Educational objectives: By the end of this education session, participants should be able to:Identify relevant airway anatomy during intubation, including base of the tongue, epiglottis, midline vallecular fold, anterior arytenoids.Appreciate the value of a stepwise anatomically guided approach to intubation.Become familiar with the midline vallecular fold and underlying anatomy, including the hyoepiglottic ligament, and how proper placement of the laryngoscope can result in improved glottic visualization.
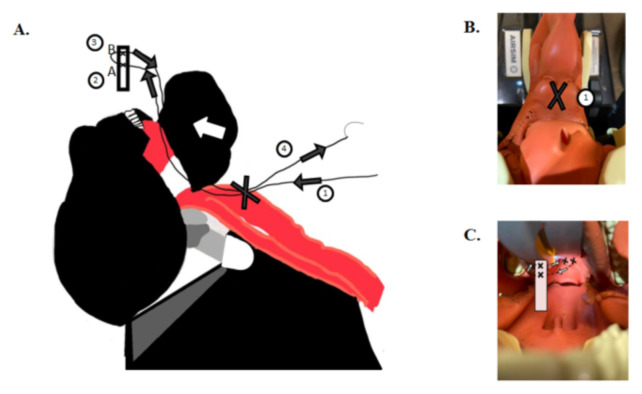
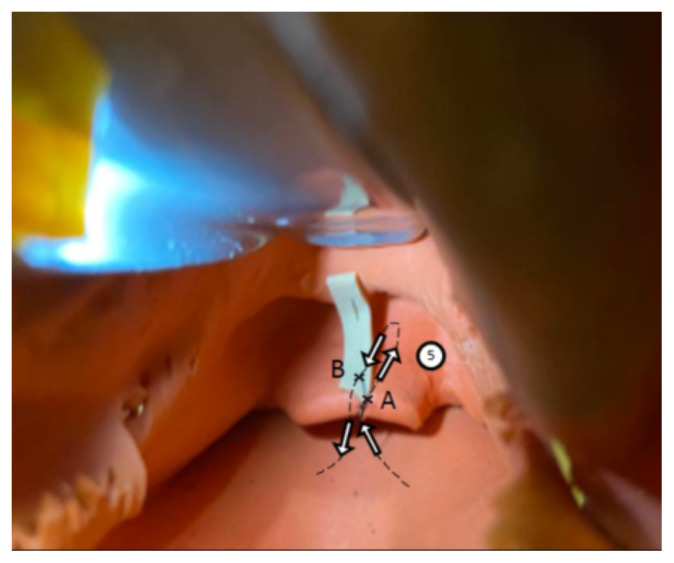
Educational methods: The TrueCorp AirSim airway task trainer was modified with the addition of a simulated MVF. Prior to the modification described here, there were no dynamic trainers with the functional fidelity needed to teach trainees how to engage the MVF with proper placement of the distal tip of the laryngoscope. Once the trainer was created, learners are introduced to relevant anatomy through the initial lecture to unsure baseline knowledge. During the lecture, videos and images are reviewed to demonstrate the importance of an anatomical roadmap to successful intubation. Learners then practiced with the modified task trainer to gain hands-on experience with laryngoscope placement and improved glottic visualization. A short verbal debriefing was performed at the end of the skills session to address any remaining questions.
Research methods: Pre- and post-simulation surveys were completed by attendees of a weekly didactic session, ranging from medical students, PGY 1-4 emergency medicine residents, and emergency medicine attending physicians. Pre- and post-simulation familiarity with airway anatomy and comfortability with MVF engagement was assessed using a 5-point Likert scale.
Results: Twenty-six participants ranging from medical students to attending physicians completed a pre- and post-simulation survey. Overall, feedback from leaners was positive. Learners were excited to learn new airway management techniques and requested an expansion of current airway curriculum based on the success of this implementation.
Discussion: This modified task trainer places an emphasis on teaching airway anatomy to trainees with the addition of functional fidelity by adding an engageable element providing the trainee with feedback on successful placement of the laryngoscope. This simple and cost-effective modification can add value to existing airway management curriculums by serving as a visual cue of airway anatomy and instructing trainees on proper placement of the laryngoscope. Our results showed participants experienced increased comfort with airway anatomy recognition and engagement of MVF for difficult intubations. Participants found the trainer effective with the simulated MVF resulting in glottic elevation and recommended this for future simulation. Participants were eager to learn additional airway techniques to improve their laryngoscopy skills, suggesting an area of growth for emergency medicine didactic curriculums.
Topics: Airway, midline vallecular fold, anatomy, difficult airway, education.
© 2024 Tumminello, et al.
Figures
Similar articles
-
An Innovative Inexpensive Portable Pulmonary Edema Intubation Simulator.J Educ Teach Emerg Med. 2020 Apr 15;5(2):I9-I20. doi: 10.21980/J8MM1R. eCollection 2020 Apr. J Educ Teach Emerg Med. 2020. PMID: 37465400 Free PMC article.
-
Innovations in Airway Education: 3D Printed Neonatal and Pediatric Needle Cricothyrotomy Trainers.J Educ Teach Emerg Med. 2020 Apr 15;5(2):I1-I8. doi: 10.21980/J8R928. eCollection 2020 Apr. J Educ Teach Emerg Med. 2020. PMID: 37465404 Free PMC article.
-
Low Fidelity Trainer for Fiberoptic Scope Use in the Emergency Department.J Educ Teach Emerg Med. 2020 Jul 15;5(3):I1-I8. doi: 10.21980/J8764B. eCollection 2020 Jul. J Educ Teach Emerg Med. 2020. PMID: 37465221 Free PMC article.
-
Low-Cost Otolaryngology Simulation Models for Early-Stage Trainees: A Scoping Review.Res Sq [Preprint]. 2023 Dec 8:rs.3.rs-3673832. doi: 10.21203/rs.3.rs-3673832/v1. Res Sq. 2023. Update in: BMC Med Educ. 2024 May 1;24(1):483. doi: 10.1186/s12909-024-05466-3. PMID: 38106212 Free PMC article. Updated. Preprint.
-
Approaches to neonatal intubation training: A scoping review.Resusc Plus. 2024 Sep 23;20:100776. doi: 10.1016/j.resplu.2024.100776. eCollection 2024 Dec. Resusc Plus. 2024. PMID: 39376638 Free PMC article.
References
-
- Kovacs G, Law A. Airway Management in Emergencies. The Infinity Edition; Excerpt from airway physiology and anatomy: a deep dive chapter in airway management in emergencies, the infinity edition. At: https://www.aimeairway.ca/book#/
-
- Barnicle R, Bracey A, Weingart S. Identifying and correcting the performance errors of video laryngoscopy: The next step in emergency airway education. SAEM Pulse. 2022;37(4):8–11.