

Evaluating process and effectiveness of a low-intensity CBT intervention for women with gynaecological cancer (the EPELIT Trial)
- PMID: 38708072
- PMCID: PMC11064984
- DOI: 10.12688/amrcopenres.12971.1
Evaluating process and effectiveness of a low-intensity CBT intervention for women with gynaecological cancer (the EPELIT Trial)
Abstract
Background: Improving survival from gynaecological cancers is creating an increasing clinical challenge for long-term distress management. Psychologist-led interventions for cancer survivors can be beneficial, but are often costly. The rise of the Psychological Wellbeing Practitioner (PWP) workforce in the UK might offer a cheaper, but equally effective, intervention delivery method that is more sustainable and accessible. We aimed to test the effectiveness of a PWP co-facilitated intervention for reducing depression and anxiety, quality of life and unmet needs.
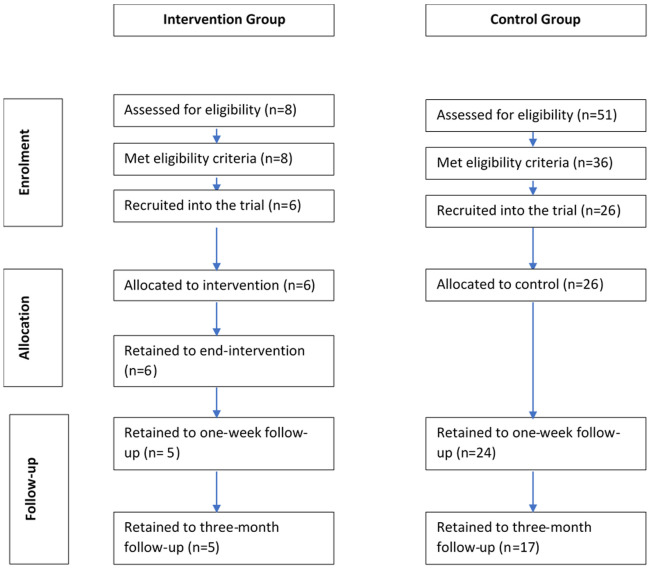
Methods: We planned this trial using a pragmatic, non-randomised controlled design, recruiting a comparator sample from a second clinical site. The intervention was delivered over six-weekly sessions; data were collected from participants at baseline, weekly during the intervention, and at one-week and three-month follow-up. Logistical challenges meant that we only recruited 8 participants to the intervention group, and 26 participants to the control group.
Results: We did not find significant, between-group differences for depression, quality of life or unmet needs, though some differences at follow-up were found for anxiety ( p<.001). Analysis of potential intervention mediator processes indicated the potential importance of self-management self-efficacy. Low uptake into the psychological intervention raises questions about (a) patient-driven needs for group-based support, and (b) the sustainability of this intervention programme.
Conclusions: This study failed to recruit to target; the under-powered analysis likely explains the lack of significant effects reported, though some trends in the data are of interest. Retention in the intervention group, and low attrition in the control group indicate acceptability of the intervention content and trial design; however a small baseline population rendered this trial infeasible in its current design. Further work is required to answer our research questions, but also, importantly, to address low uptake for psychological interventions in this group of cancer survivors.
Trial registration: ClinicalTrials.gov, NCT03553784 (registered 14 June 2018).
Keywords: Gynaecological cancer; anxiety; cognitive behavioural therapy; depression; distress; low-intensity; quality of life; unmet needs.
Plain language summary
An increasing number of people are surviving for longer time periods following treatment for gynaecological cancer and this means we need to change how we care for and support a growing cancer survivor population. Psychological distress and poor quality of life are common in people affected by cancer, and these do not always improve once treatment ends. Providing psychological support can be expensive, which means that not everyone who wants it can access it. Psychological Wellbeing Practitioners (PWPs) have been introduced in UK health care. This workforce might offer an alternative for providing psychological support to a greater number of cancer survivors. We aimed to test how good a PWP co-delivered intervention is at improving depression, anxiety and quality of life in people who had been treated for gynaecological cancer. The intervention was delivered to small groups of patients over six weekly sessions. We compared those who received the intervention with a similar patient group who did not have access to the same psychological support from a different hospital. Participants reported their psychological wellbeing and quality of life at the point of recruitment, weekly for six weeks, and then at follow-up time-points one week and three months later. Because of low interest in the group intervention we did not recruit to target. Only 8 participants took part in the intervention, and we recruited only 26 participants in the control group. This means we can’t have full confidence in our results. Nonetheless, the findings indicate that this intervention was helpful for improving participants’ anxiety levels. Further trials, which recruit a larger number of cancer survivors, are needed to answer our research questions. However, this trial indicates acceptability and potential benefit. We also need to undertake research to understand why so few cancer survivors wanted to take part in this group-based intervention.
Copyright: © 2021 Hulbert-Williams NJ et al.
Conflict of interest statement
No competing interests were disclosed.
Figures
References
-
- Office for National Statistics: Cancer registration statistics, England: 2017. Reference Source
-
- Youlden D, Coory M, Baade PD: Cancer Survival in Queensland 2002.Brisbane, Queensland Health and Queensland Fund; 2005. Reference Source
-
- Coleman MP, Forman D, Bryant H, et al. : Cancer survival in Australia, Canada, Denmark, Norway, Sweden, and the UK 1995-2007 (the International Cancer Benchmarking Partnership): an analysis of population-based cancer registry data. Lancet. 2011;377(9760):127–138. 10.1016/S0140-6736(10)62231-3 - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical