

Early Cold Stored Platelet Transfusion Following Severe Injury: A Randomized Clinical Trial
- PMID: 38708880
- PMCID: PMC11224567
- DOI: 10.1097/SLA.0000000000006317
Early Cold Stored Platelet Transfusion Following Severe Injury: A Randomized Clinical Trial
Abstract
Objective: To determine the feasibility, efficacy, and safety of early cold stored platelet transfusion compared with standard care resuscitation in patients with hemorrhagic shock.
Background: Data demonstrating the safety and efficacy of early cold stored platelet transfusion are lacking following severe injury.
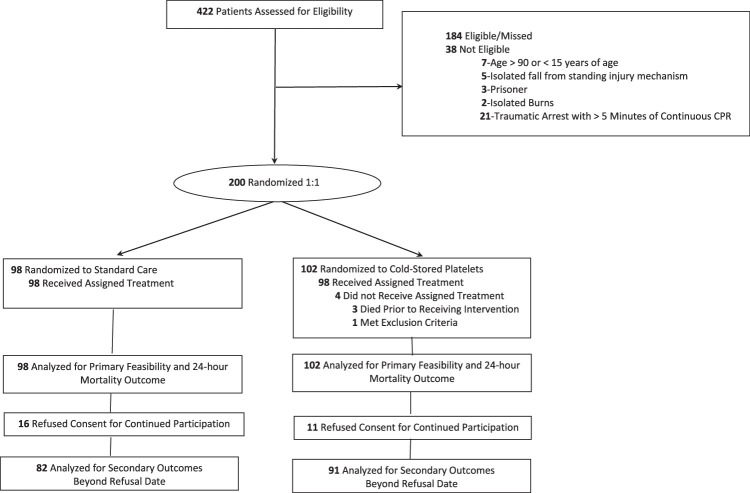
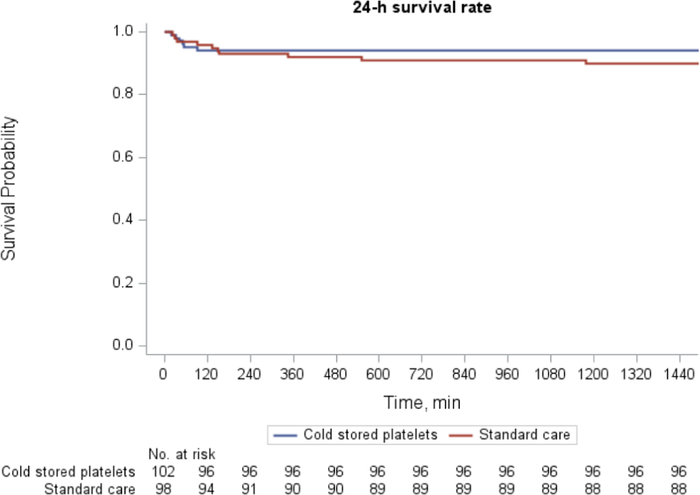
Methods: A phase 2, multicenter, randomized, open label, clinical trial was performed at 5 US trauma centers. Injured patients at risk of large volume blood transfusion and the need for hemorrhage control procedures were enrolled and randomized. The intervention was the early transfusion of a single apheresis cold stored platelet unit, stored for up to 14 days versus standard care resuscitation. The primary outcome was feasibility and the principal clinical outcome for efficacy and safety was 24-hour mortality.
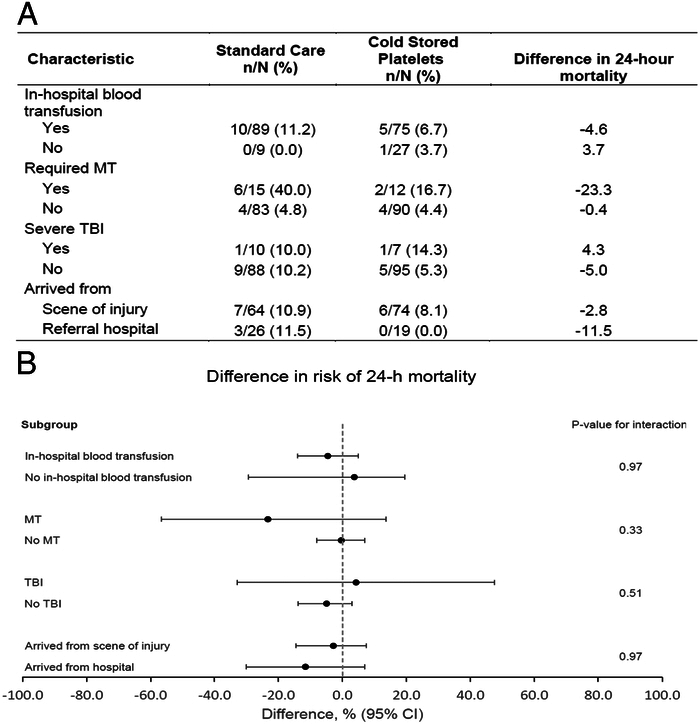
Results: Mortality at 24 hours was 5.9% in patients who were randomized to early cold stored platelet transfusion compared with 10.2% in the standard care arm (difference, -4.3%; 95% CI, -12.8% to 3.5%; P =0.26). No significant differences were found for any of the prespecified ancillary outcomes. Rates of arterial and/or venous thromboembolism and adverse events did not differ across treatment groups.
Conclusions and relevance: In severely injured patients, early cold stored platelet transfusion is feasible, safe and did not result in a significant lower rate of 24-hour mortality. Early cold stored platelet transfusion did not result in a higher incidence of arterial and/or venous thrombotic complications or adverse events. The storage age of the cold stored platelet product was not associated with significant outcome differences.
Trial registration: ClinicalTrials.gov identifier: NCT04667468.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
J.L.S. reports grants from the DoD; F.X.G. reports grants from the DoD; S.R.W. reports grants from the DoD; L.Z.K. reports grants and consulting fees from University of Maryland/BARDA, personal fees from Gamma Diagnostics, Coagulant Therapeutics, Haemonetics, other from Cerus, outside the submitted work; A.E.K. reports being founder of CaptureDx; J.C. reports participates on the steering committee for Faraday Pharmaceuticals; M.D.N. has received grants from National Institutes of Health, Department of Defense, DARPA, Haemonetics, Alexion and Instrumentation Laboratories, honoraria for lectures from Haemonetics and Takeda, support for attending meetings and/or travel from Takeda; participates on a Data Safety Monitoring Board or Advisory Board from NHLBI CONNECTS Steering Committee; is the Chief Medical Officer, Haima Therapeutics, and has Patents planned, issued or pending (US Patent 11,408.844; US Patent 9.072,760), outside the submitted work; P.C.S. reports personal fees from Hemanext, Cerus, participates in advisory board for Octapharma,and Haima, and is the Co-Founder and Chief Medical Officer of Kalocyte, outside the submitted work. The remaining authors report no conflicts of interest.
Figures
References
-
- Cannon JW. Hemorrhagic shock. N Engl J Med. 2018;378:370–379. - PubMed
-
- Davis JS, Satahoo SS, Butler FK, et al. An analysis of prehospital deaths: Who can we save? J Trauma Acute Care Surg. 2014;77:213–218. - PubMed
-
- Eastridge BJ, Mabry RL, Seguin P, et al. Death on the battlefield (2001-2011): implications for the future of combat casualty care. J Trauma Acute Care Surg. 2012;73(suppl 5):S431–S437. - PubMed
-
- Rhee P, Joseph B, Pandit V, et al. Increasing trauma deaths in the United States. Ann Surg. 2014;260:13–21. - PubMed
