

Robotic transanal minimally invasive surgery (r-TAMIS): perioperative and short-term outcomes for local excision of rectal cancers
- PMID: 38710889
- PMCID: PMC11133047
- DOI: 10.1007/s00464-024-10829-4
Robotic transanal minimally invasive surgery (r-TAMIS): perioperative and short-term outcomes for local excision of rectal cancers
Abstract
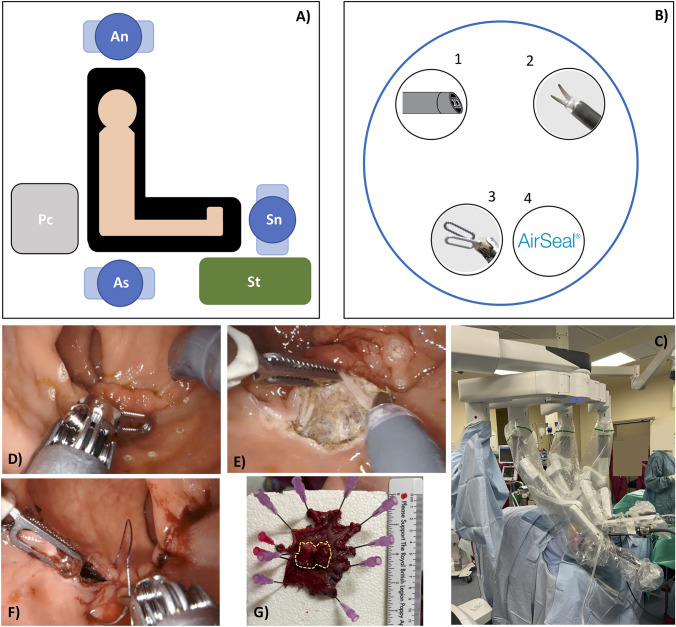
Background: Transanal minimally invasive surgery (TAMIS) is an advanced technique for excision of early rectal cancers. Robotic TAMIS (r-TAMIS) has been introduced as technical improvement and potential alternative to total mesorectal excision (TME) in early rectal cancers and in frail patients. This study reports the perioperative and short-term oncological outcomes of r-TAMIS for local excision of early-stage rectal cancers.
Methods: Retrospective analysis of a prospectively collected r-TAMIS database (July 2021-July 2023). Demographics, clinicopathological features, short-term outcomes, recurrences, and survival were investigated.
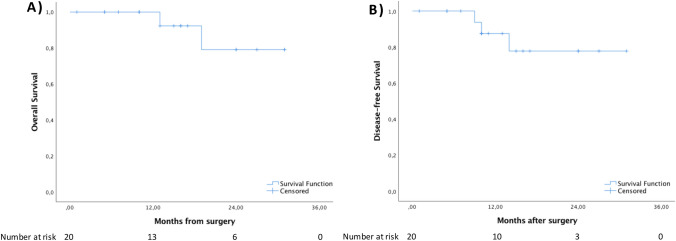
Results: Twenty patients were included. Median age and body mass index were 69.5 (62.0-77.7) years and 31.0 (21.0-36.5) kg/m2. Male sex was prevalent (n = 12, 60.0%). ASA III accounted for 66.7%. Median distance from anal verge was 7.5 (5.0-11.7) cm. Median operation time was 90.0 (60.0-112.5) minutes. Blood loss was minimal. There were no conversions. Median postoperative stay was 2.0 (1.0-3.0) days. Minor and major complication rates were 25.0% and 0%, respectively. Seventeen (85.0%) patients had an adenocarcinoma whilst three patients had an adenoma. R0 rate was 90.0%. Most tumours were pT1 (55.0%), followed by pT2 (25.0%). One patient (5.0%) had a pT3 tumour. Specimen and tumour maximal median diameter were 51.0 (41.0-62.0) mm and 21.5 (17.2-42.0) mm, respectively. Median specimen area was 193.1 (134.3-323.3) cm2. Median follow-up was 15.5 (10.0-24.0) months. One patient developed local recurrence (5.0%).
Conclusions: r-TAMIS, with strict postoperative surveillance, is a safe and feasible approach for local excision of early rectal cancer and may have a role in surgically unfit and elderly patients who refuse or cannot undergo TME surgery. Future prospective multicentre large-scale studies are needed to report the long-term oncological outcomes.
Keywords: Rectal cancer; Robotic surgery; Robotic transanal surgery; TAMIS; Total mesorectal excision.
© 2024. Crown.
Conflict of interest statement
Jim Khan performs proctoring for Intuitive Surgical and educational activity with Johnson & Johnson. Guglielmo Niccolò Piozzi, Ania Przedlacka, Rauand Duhoky, Oroog Ali, Yasser Ghanem, Richard Beable, and Tony Higginson have no conflicts of interest to disclose.
Figures
References
-
- Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986;1:1479–1482. - PubMed
-
- Guren MG, Eriksen MT, Wiig JN, Carlsen E, Nesbakken A, Sigurdsson HK, et al. Quality of life and functional outcome following anterior or abdominoperineal resection for rectal cancer. Eur J Surg Oncol. 2005;31:735–742. - PubMed
-
- Dinnewitzer A, Jager T, Nawara C, Buchner S, Wolfgang H, Ofner D. Cumulative incidence of permanent stoma after sphincter preserving low anterior resection of mid and low rectal cancer. Dis Colon Rectum. 2013;56:1134–1142. - PubMed
-
- Borowski DW, Bradburn DM, Mills SJ, Bharathan B, Wilson RG, Ratcliffe AA, et al. Volume-outcome analysis of colorectal cancer-related outcomes. Br J Surg. 2010;97:1416–1430. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
