

Myopia Control: Are We Ready for an Evidence Based Approach?
- PMID: 38710983
- PMCID: PMC11109072
- DOI: 10.1007/s40123-024-00951-w
Myopia Control: Are We Ready for an Evidence Based Approach?
Abstract
Introduction: Myopia and its vision-threatening complications present a significant public health problem. This review aims to provide an updated overview of the multitude of known and emerging interventions to control myopia, including their potential effect, safety, and costs.
Methods: A systematic literature search of three databases was conducted. Interventions were grouped into four categories: environmental/behavioral (outdoor time, near work), pharmacological (e.g., atropine), optical interventions (spectacles and contact lenses), and novel approaches such as red-light (RLRL) therapies. Review articles and original articles on randomized controlled trials (RCT) were selected.
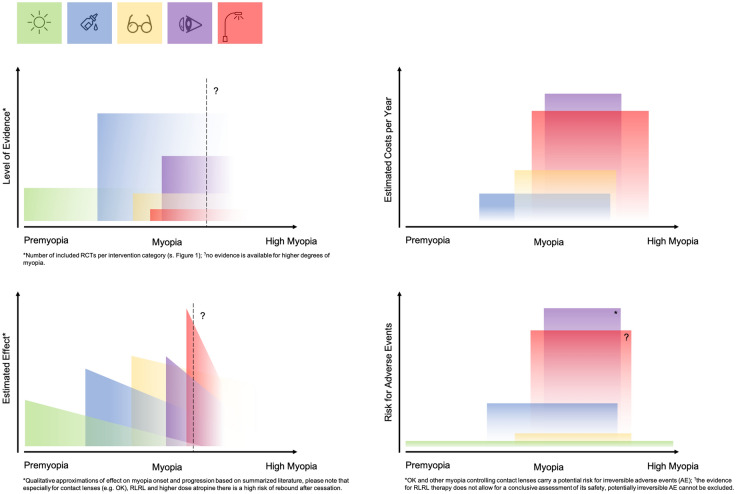
Results: From the initial 3224 retrieved records, 18 reviews and 41 original articles reporting results from RCTs were included. While there is more evidence supporting the efficacy of low-dose atropine and certain myopia-controlling contact lenses in slowing myopia progression, the evidence about the efficacy of the newer interventions, such as spectacle lenses (e.g., defocus incorporated multiple segments and highly aspheric lenslets) is more limited. Behavioral interventions, i.e., increased outdoor time, seem effective for preventing the onset of myopia if implemented successfully in schools and homes. While environmental interventions and spectacles are regarded as generally safe, pharmacological interventions, contact lenses, and RLRL may be associated with adverse effects. All interventions, except for behavioral change, are tied to moderate to high expenditures.
Conclusion: Our review suggests that myopia control interventions are recommended and prescribed on the basis of accessibility and clinical practice patterns, which vary widely around the world. Clinical trials indicate short- to medium-term efficacy in reducing myopia progression for various interventions, but none have demonstrated long-term effectiveness in preventing high myopia and potential complications in adulthood. There is an unmet need for a unified consensus for strategies that balance risk and effectiveness for these methods for personalized myopia management.
Keywords: Cost; Effect; Intervention; Myopia control; Myopia management; RCTs; Safety.
© 2024. The Author(s).
Conflict of interest statement
Andrzej Grzybowski is an Editorial Board member of
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
