Association between pre-biologic T2-biomarker combinations and response to biologics in patients with severe asthma
- PMID: 38711495
- PMCID: PMC11070939
- DOI: 10.3389/fimmu.2024.1361891
Association between pre-biologic T2-biomarker combinations and response to biologics in patients with severe asthma
Abstract
Background: To date, studies investigating the association between pre-biologic biomarker levels and post-biologic outcomes have been limited to single biomarkers and assessment of biologic efficacy from structured clinical trials.
Aim: To elucidate the associations of pre-biologic individual biomarker levels or their combinations with pre-to-post biologic changes in asthma outcomes in real-life.
Methods: This was a registry-based, cohort study using data from 23 countries, which shared data with the International Severe Asthma Registry (May 2017-February 2023). The investigated biomarkers (highest pre-biologic levels) were immunoglobulin E (IgE), blood eosinophil count (BEC) and fractional exhaled nitric oxide (FeNO). Pre- to approximately 12-month post-biologic change for each of three asthma outcome domains (i.e. exacerbation rate, symptom control and lung function), and the association of this change with pre-biologic biomarkers was investigated for individual and combined biomarkers.
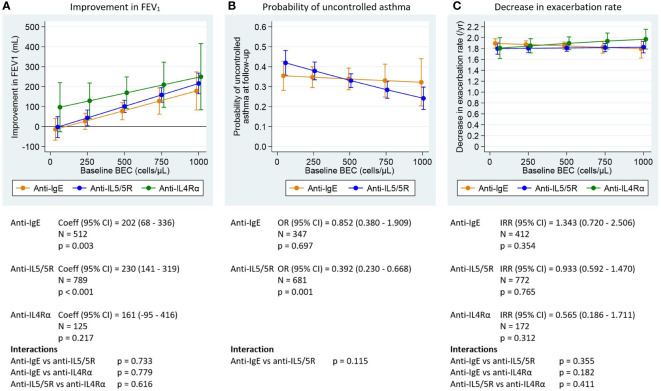
Results: Overall, 3751 patients initiated biologics and were included in the analysis. No association was found between pre-biologic BEC and pre-to-post biologic change in exacerbation rate for any biologic class. However, higher pre-biologic BEC and FeNO were both associated with greater post-biologic improvement in FEV1 for both anti-IgE and anti-IL5/5R, with a trend for anti-IL4Rα. Mean FEV1 improved by 27-178 mL post-anti-IgE as pre-biologic BEC increased (250 to 1000 cells/µL), and by 43-216 mL and 129-250 mL post-anti-IL5/5R and -anti-IL4Rα, respectively along the same BEC gradient. Corresponding improvements along a FeNO gradient (25-100 ppb) were 41-274 mL, 69-207 mL and 148-224 mL for anti-IgE, anti-IL5/5R, and anti-IL4Rα, respectively. Higher baseline BEC was also associated with lower probability of uncontrolled asthma (OR 0.392; p=0.001) post-biologic for anti-IL5/5R. Pre-biologic IgE was a poor predictor of subsequent pre-to-post-biologic change for all outcomes assessed for all biologics. The combination of BEC + FeNO marginally improved the prediction of post-biologic FEV1 increase (adjusted R2: 0.751), compared to BEC (adjusted R2: 0.747) or FeNO alone (adjusted R2: 0.743) (p=0.005 and <0.001, respectively); however, this prediction was not improved by the addition of IgE.
Conclusions: The ability of higher baseline BEC, FeNO and their combination to predict biologic-associated lung function improvement may encourage earlier intervention in patients with impaired lung function or at risk of accelerated lung function decline.
Keywords: FEV1; FeNO (Fraction of exhaled Nitric Oxide); biologics; biomarkers; eosinophil (EOS); personalized medicine (PM); severe asthma.
Copyright © 2024 Porsbjerg, Townend, Bergeron, Christoff, Katsoulotos, Larenas-Linnemann, Tran, Al-Lehebi, Bosnic-Anticevich, Busby, Hew, Kostikas, Papadopoulos, Pfeffer, Popov, Rhee, Sadatsafavi, Tsai, Ulrik, Al-Ahmad, Altraja, Beastall, Bulathsinhala, Carter, Cosio, Fletton, Hansen, Heaney, Hubbard, Kuna, Murray, Nagano, Pini, Cano Rosales, Schleich, Wechsler, Amaral, Bourdin, Brusselle, Chen, Chung, Denton, Fonseca, Hoyte, Jackson, Katial, Kirenga, Koh, Ławkiedraj, Lehtimäki, Liew, Mahboub, Martin, Menzies-Gow, Pang, Papaioannou, Patel, Perez-De-Llano, Peters, Ricciardi, Rodríguez-Cáceres, Solarte, Tay, Torres-Duque, Wang, Zappa, Abisheganaden, Assing, Costello, Gibson, Heffler, Máspero, Nicola, Perng (Steve), Puggioni, Salvi, Sheu, Sirena, Taillé, Tan, Bjermer, Canonica, Iwanaga, Jiménez-Maldonado, Taube, Brussino and Price.
Conflict of interest statement
CP has attended advisory boards for AstraZeneca, Novartis, TEVA, and Sanofi-Genzyme; has given lectures at meetings supported by AstraZeneca, Novartis, TEVA, Sanofi-Genzyme, and GlaxoSmithKline; has taken part in clinical trials sponsored by AstraZeneca, Novartis, MSD, Sanofi-Genzyme, GlaxoSmithKline, and Novartis; and has received educational and research grants from AstraZeneca, Novartis, TEVA, GlaxoSmithKline, ALK, and Sanofi-Genzyme. JT is an employee of the Observational and Pragmatic Research Institute OPRI. OPRI conducted this study in collaboration with Optimum Patient Care and AstraZeneca. CB reports advisory board participation of Sanofi-Regeneron, AstraZeneca, Takeda, ValeoPharma, honorarium for presentations for AstraZeneca/Amgen, GlaxoSmithKline, Grifols, Sanofi-Regeneron, ValeoPharma and grants paid to UBC from BioHaven, Sanofi-Regeneron, AstraZeneca, GlaxoSmithKline. GCC declares relevant research support from AstraZeneca and Sanofi. GK has attended advisory boards for AstraZeneca, GlaxoSmithKline and Chiesi. He has also given lectures at meetings supported by Novartis, Sanofi-Genzyme, AstraZeneca, GlaxoSmithKline, and Boehringer-Ingelheim. DL reports personal fees from ALK-Abelló, AstraZeneca national and global, Bayer, Chiesi, Grunenthal, Grin, GlaxoSmithKline national and global, Viatris, Menarini, MSD, Novartis, Pfizer, Sanofi, Siegfried, UCB, Carnot, grants from Abbvie, Bayer, Lilly, Sanofi, AstraZeneca, Pfizer, Novartis, Circassia, UCB, GlaxoSmithKline, outside the submitted work. TNT is an employee of AstraZeneca and may own stock or stock options in AstraZeneca. AstraZeneca is a co-funder of ISAR. RA-L has given lectures at meetings supported by AstraZeneca, Boehringer Ingelheim, Novartis, GlaxoSmithKline, and Sanofi, and participated in advisory board fees from GlaxoSmithKline, AstraZeneca, Novartis, and Abbott. SB-A has received honorarium for participation in expert advisory boards and given lectures for Teva Pharmaceuticals, AstraZeneca, GlaxoSmithKline, Meda, Mundipharma, Sanofi, Mylan and received unrestricted research grants from Mylan, AstraZeneca, Teva, Mundipharma International, GlaxoSmithKline, and Viatris. JB has received research grants from AstraZeneca and personnel fees from NuvoAir, outside the submitted work. MH declares grants and other advisory board fees made to his institutional employer from AstraZeneca, GlaxoSmithKline, Novartis, Sanofi, Teva, and Seqirus, for unrelated projects. KK received honoraria for presentations and consultancy fees from AstraZeneca, Boehringer Ingelheim, CSL Behring, Chiesi, ELPEN, Gilead, GlaxoSmithKline, Menarini, Novartis, Sanofi, Specialty Therapeutics, WebMD. His department has received funding and grants from AstraZeneca, Boehringer Ingelheim, Chiesi, Innovis, ELPEN, GlaxoSmithKline, Menarini, Novartis and NuvoAir. NP has been a speaker and/or advisory board member for Abbott, Abbvie, ALK, Asit Biotech, AstraZeneca, Biomay, Boehringer Ingelheim, GlaxoSmithKline, HAL, Faes Farma, Medscape, Menarini, MSD, Novartis, Nutricia, OM Pharma, Regeneron, Sanofi, Takeda, and Viatris. PEP has attended advisory boards for AstraZeneca, GlaxoSmithKline, and Sanofi; has given lectures/webinars at meetings supported by AstraZeneca, Chiesi and GlaxoSmithKline; has taken part in clinical trials sponsored by AstraZeneca, GlaxoSmithKline, Novartis, Regeneron, and Sanofi, for which his institution received remuneration; and has a current research grant funded by GlaxoSmithKline. TP declares relevant research support from Novartis and Chiesi Pharma. CR received consulting/lecture fees from MSD, AstraZeneca, GlaxoSmithKline, Novartis, Takeda, Mundipharma, Boehringer-Ingelheim, Teva, Sanofi, and Bayer. MS has received honoraria from AstraZeneca, Boehringer Ingelheim, Teva, and GlaxoSmithKline for purposes unrelated to the content of this manuscript and has received research funding from AstraZeneca and Boehringer Ingelheim directly into his research account from AstraZeneca for unrelated projects. M-JT has received sponsorship to attend or speak at conferences, honoraria for lecturing or attending advisory boards, and research grants from the following companies: AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Pfizer, Shionogi and Orient EuroPharma. CU reports personal fees for talks, participation in advisory boards etc. from AstraZeneca, GlaxoSmithKline, Teva, Boehringer Ingelheim, Orion Pharma, Sanofi Genzyme, TFF Pharmaceuticals, Covis Pharma, Berlin-Chemie, Takeda, Chiesi, and Pfizer, outside the submitted work. MA-A has received advisory board and speaker fees from AstraZeneca, Sanofi, Novartis, and GlaxoSmithKline and received a grant from Kuwait Foundation for the Advancement of Sciences KFAS. AA has received lecture fees from AstraZeneca, Berlin-Chemie Menarini, Boehringer Ingelheim, CSL Behring, GlaxoSmithKline, MSD, Norameda, Novartis, Orion, Sanofi, and Zentiva; sponsorships from AstraZeneca, Berlin-Chemie Menarini, Boehringer Ingelheim, GlaxoSmithKline, MSD, Norameda, Novartis, and Sanofi; and has participated in advisory boards for AstraZeneca, Boehringer Ingelheim, CSL Behring, GlaxoSmithKline, MSD, Novartis, Sanofi, and Teva. ABe is an employee of Optimum Patient Care Global, a co-funder of the International Severe Asthma Registry. LBu is an employee of the Observational and Pragmatic Research Institute OPRI. OPRI conducted this study in collaboration with Optimum Patient Care and AstraZeneca. VC is an employee of Optimum Patient Care OPC. OPC is a co-funder of the International Severe Asthma Registry. BC declares grants from Chiesi and GlaxoSmithKline; personal fees for advisory board activities from Chiesi, GlaxoSmithKline, Novartis, Sanofi, Teva, and AstraZeneca; and payment for lectures/speaking engagements from Chiesi, Novartis, GlaxoSmithKline, Menarini, and AstraZeneca, outside the submitted work. KF is an employee of Optimum Patient Care Global OPCG, a co-funder of the International Severe Asthma Registry. LH has received grant funding, participated in advisory boards and given lectures at meetings supported by Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Circassia, Hoffmann la Roche, GlaxoSmithKline, Novartis, Theravance, Evelo Biosciences, Sanofi, and Teva; he has received grants from MedImmune, Novartis UK, Roche/Genentech Inc, and GlaxoSmithKline, Amgen, Genentech/Hoffman la Roche, AstraZeneca, MedImmune, GlaxoSmithKline, Aerocrine, and Vitalograph; he has received sponsorship for attending international scientific meetings from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, and Napp Pharmaceuticals; he has also taken part in asthma clinical trials sponsored by AstraZeneca, Boehringer Ingelheim, Hoffmann la Roche, and GlaxoSmithKline for which his institution received remuneration; he is the Academic Lead for the Medical Research Council Stratified Medicine UK Consortium in Severe Asthma which involves industrial partnerships with a number of pharmaceutical companies including Amgen, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Hoffmann la Roche, and Janssen. RH is an employee for Observational and Pragmatic Research Institute OPRI which conducted this study in collaboration with Optimum Patient Care and AstraZeneca. PK reports personal fees from Adamed, AstraZeneca, Berlin Chemie Menarini, FAES, Glenmark, Novartis, Polpharma, Boehringer Ingelheim, Teva, Zentiva, outside the submitted work. RM is a consultant for Observational and Pragmatic Research Institute OPRI which conducted this study in collaboration with Optimum Patient Care and AstraZeneca. TN received lecture fees from Kyorin, GlaxoSmithKline, Novartis, Sanofi, and AstraZeneca. LP received research grants and lecture fees from GlaxoSmithKline, Menarini, Chiesi, AstraZeneca and Grifols. DC has received speaker fees from AstraZeneca, Boehringer Ingelheim, and has acted as an investigator for trials sponsored by AstraZeneca. FS reports consultancy work for GlaxoSmithKline, AstraZeneca, Sanofi - Advisory board, received speaker fees from GlaxoSmithKline, AstraZeneca, Chiesi, Amgen, Teva and research grants from GlaxoSmithKline, AstraZeneca, and Chiesi. MW reports grants and/or personal fees from Novartis, Sanofi, Regeneron, Genentech, Sentien, Restorbio, Equillium, Genzyme, Cohero Health, Teva, Boehringer Ingelheim, AstraZeneca, Amgen, GlaxoSmithKline, Cytoreason, Cerecor, Sound Biologics, Incyte, and Kinaset. ABo has received industry-sponsored grants from AstraZeneca/MedImmune, Boehringer-Ingelheim, Cephalon/Teva, GlaxoSmithKline, Novartis, Sanofi-Regeneron, and consultancies with AstraZeneca/MedImmune, Boehringer-Ingelheim, GlaxoSmithKline, Novartis, Regeneron-Sanofi, Med-in-Cell, Actelion, Merck, Roche, and Chiesi. GB has received honoraria for lectures from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, and Novartis. He is a member of advisory boards for AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, MSD Merck sharp & Dohme, Novartis, and Sanofi/Regeneron. LC has received speaker and consultancy fees and conference expenses from AstraZeneca, Novartis, GlaxoSmithKline, Boehringer Ingelheim and Menarini. ED declares grants to her institution from AstraZeneca, GlaxoSmithKline, Novartis, Sanofi, Teva, and Seqirus, for unrelated projects and speaker fees from Sanofi. JF reports grants from research agreements with AstraZeneca, Mundipharma, Sanofi Regeneron, and Novartis. Personal fees for lectures and attending advisory boards: AstraZeneca, GlaxoSmithKline, Mundipharma, Novartis, Sanofi Regeneron, and Teva. FH declares honoraria from AstraZeneca, Sanofi, TEVA, GSK, and Genentech. She has been an investigator on clinical trials sponsored by GlaxoSmithKline, Genentech, and Sanofi, for which her institution has received funding. DJ has received speaker fees and consultancy fees from AstraZeneca, GlaxoSmithKline, Sanofi Regeneron, Boehringer Ingelheim and research funding from AstraZeneca. MK reports grant support from AstraZeneca, and honoraria for lectures and advisory board meetings paid to her hospital Singapore General Hospital from GlaxoSmithKline, AstraZeneca, Novartis, Sanofi and Boehringer Ingelheim, outside the submitted work. LL has received personal fees from ALK, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Menarini, Novartis, Orion Pharma and Sanofi. NM is an employee of AstraZeneca and may own stock or stock options in AstraZeneca. AstraZeneca is a co-funder of ISAR. AM-G is an employee of AstraZeneca and may own stock or stock options in AstraZeneca. AstraZeneca is a co-funder of ISAR. PHwP has received honoraria for talks and advisory board meetings from GlaxoSmithKline, AstraZeneca, and Sanofi. AP has received fees and honoraria from Menarini, GlaxoSmithKline, Novartis, Elpen, Boehringer Ingelheim, AstraZeneca, and Chiesi. PHP has received advisory board and speaker fees from AstraZeneca, GlaxoSmithKline, Novartis, and Sanofi/Regeneron. LP-d-L reports grants, personal fees and non-financial support from AstraZeneca, personal fees and non-financial support from GlaxoSmithKline, grants, personal fees and non-financial support from Teva, personal fees and non-financial support from Chiesi, grants, personal fees and non-financial support from Sanofi, personal fees from MSD, personal fees from Techdow Pharma, grants, personal fees and non-financial support from Faes Farma, personal fees from Leo-Pharma, grants and personal fees from Gebro, personal fees from Gilead, outside the submitted work. MP declares personal fees and non-financial support from AstraZeneca, GlaxoSmithKline, and Sanofi. LR received fees as a speaker from AstraZeneca, GlaxoSmithKline, Novartis, and Sanofi. IS has received fees as advisory board participant and/or speaker from GlaxoSmithKline and Sanofi. CT-D has received fees as advisory board participant and/or speaker from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Novartis, and Sanofi-Aventis; has taken part in clinical trials from AstraZeneca, Novartis, and Sanofi-Aventis; has received unrestricted grants for investigator-initiated studies at Fundacion Neumologica Colombiana from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Grifols and Novartis. EW has received honoraria from AstraZeneca, GlaxoSmithKline, and Genentech. She has been an investigator on studies sponsored by AstraZeneca, GlaxoSmithKline, Genentech, Sanofi, Novartis, and Teva, for which her institution has received funding. RC has received honoraria for lectures from Aerogen, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Teva. He is a member of advisory boards for GlaxoSmithKline and Novartis, has received grant support from GlaxoSmithKline and Aerogen and has patents in the use of acoustics in the diagnosis of lung disease, assessment of adherence and prediction of exacerbations. PG has received speaker fees and grants to his institution from AstraZeneca, GlaxoSmithKline, and Novartis. EH declares personal fees for advisory boards participation and/or speaker activities from: Sanofi, Regeneron, GlaxoSmithKline, Novartis, AstraZeneca, Stallergenes-Greer, Circassia, Bosch, Celltrion-Healthcare, Chiesi, and Almirall. JM reports speaker fees, grants or advisory boards for AstraZeneca, Sanofi, GlaxoSmithKline, Novartis, Inmunotek, Menarini and Noucor. D-WP received sponsorship to attend or speak at international meetings, honoraria for lecturing or attending advisory boards, and research grants from the following companies: AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Daiichi Sankyo, Shionogi, and Orient Pharma. FP reports having received lectures or advisory board fees from: Menarini, Mundipharma, Chiesi, Alk Abello, AstraZeneca, Boehringer Ingelheim, Guidotti, Malesci, GlaxoSmithKline, Hal Allergy, Novartis, Sanofi, Regeneron, Stallergenes Greer, Valeas, and Almirall. SS declares research support and speaker fees from Cipla, Glenmark, and GlaxoSmithKline. C-CS has received speaker fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Pfizer, and has acted as an investigator for trials sponsored by AstraZeneca, Novartis, Roche, Sanofi-Regeneron, Galapagos, Shionogi, Aridis, Bristol Myers Squibb, Insmed, United Therapeutics, Enanta Pharmaceuticals, Areteia Therapeutics, Meiji, and Horizon Therapeutics. CT has received lecture or advisory board fees and grants to her institution from AstraZeneca, Sanofi, GlaxoSmithKline, Chiesi and Novartis, for unrelated projects. TT is an advisory Board Member for Boehringer Ingelheim, AstraZeneca, Takeda, GlaxoSmithKline, MSD, Mundipharma, and Janssen. Honoraria were received for these advisory boards. Honoraria were received for speaking at CMEs for AstraZeneca in the past. Conference sponsorships from AstraZeneca, Boehringer Ingelheim, Merck Serono, GlaxoSmithKline, Norvatis, Mundipharma and MSD. Research grants from Merck Serono Concor Study, MSD Apbord study. LBj has in the last three years received lecture or advisory board fees from Alk-Abello, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Mundipharma, Novartis, Sanofi, Genzyme/Regeneron, and Teva. GWC has received research grants, as well as lecture or advisory board fees from A. Menarini, Alk-Albello, Allergy Therapeutics, Anallergo, AstraZeneca, MedImmune, Boehringer Ingelheim, Chiesi Farmaceutici, Circassia, Danone, Faes, Genentech, Guidotti Malesci, GlaxoSmithKline, Hal Allergy, Merck, MSD, Mundipharma, Novartis, Orion, Sanofi Aventis, Sanofi, Genzyme/Regeneron, Stallergenes, UCB Pharma, Uriach Pharma, Teva, Thermo Fisher, and Valeas. TI received speaker bureau fees from Kyorin, GlaxoSmithKline, Novartis, Boehringer Ingelheim, AstraZeneca and Sanofi. LJ-M has received fees as advisory board participant and/or speaker from AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Novartis, and Sanofi-Aventis; has participated in clinical trials for AstraZeneca, Novartis, and GlaxoSmithKline. DP has advisory board membership with AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Viatris, Teva Pharmaceuticals; consultancy agreements with AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Viatris, Teva Pharmaceuticals; grants and unrestricted funding for investigator-initiated studies conducted through Observational and Pragmatic Research Institute Pte Ltd from AstraZeneca, Chiesi, Viatris, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, and UK National Health Service; payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Commune Digital, GlaxoSmithKline, Medscape, Viatris, Novartis, Regeneron Pharmaceuticals and Sanofi Genzyme, Teva Pharmaceuticals; payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Novartis, Medscape, Teva Pharmaceuticals; stock/stock options from AKL Research and Development Ltd which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd Australia and UK and 92.61% of Observational and Pragmatic Research Institute Pte Ltd Singapore; 5% shareholding in Timestamp which develops adherence monitoring technology; is peer reviewer for grant committees of the UK Efficacy and Mechanism Evaluation Programme, and Health Technology Assessment; and was an expert witness for GlaxoSmithKline. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures