

Acute and chronic eosinophilic pneumonia: an overview
- PMID: 38711783
- PMCID: PMC11070545
- DOI: 10.3389/fmed.2024.1355247
Acute and chronic eosinophilic pneumonia: an overview
Abstract
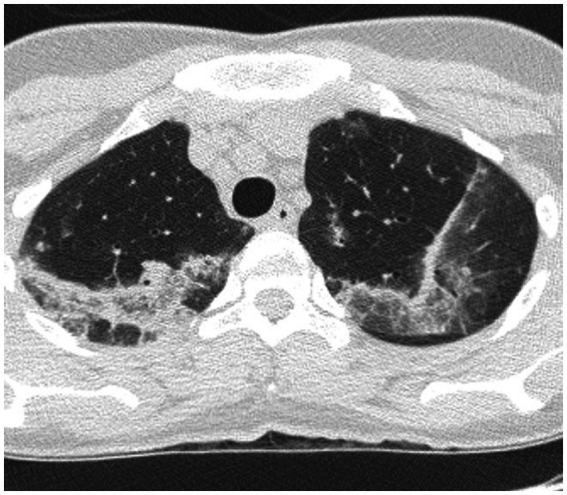
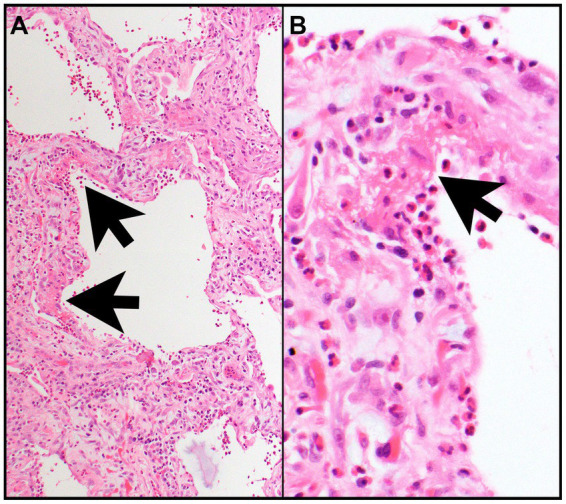
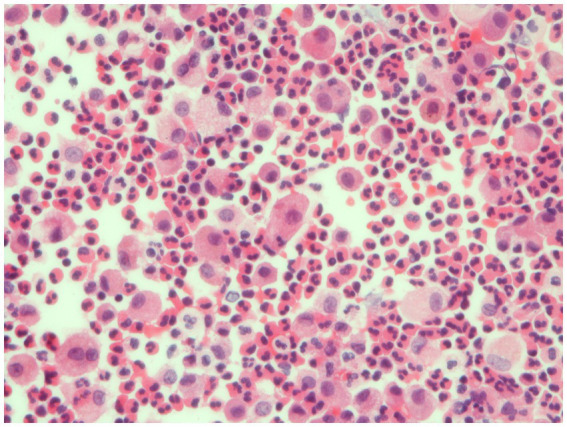
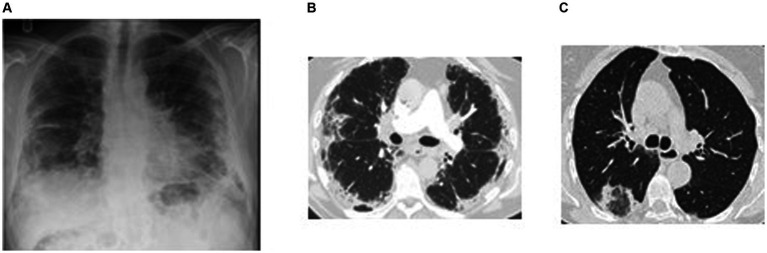
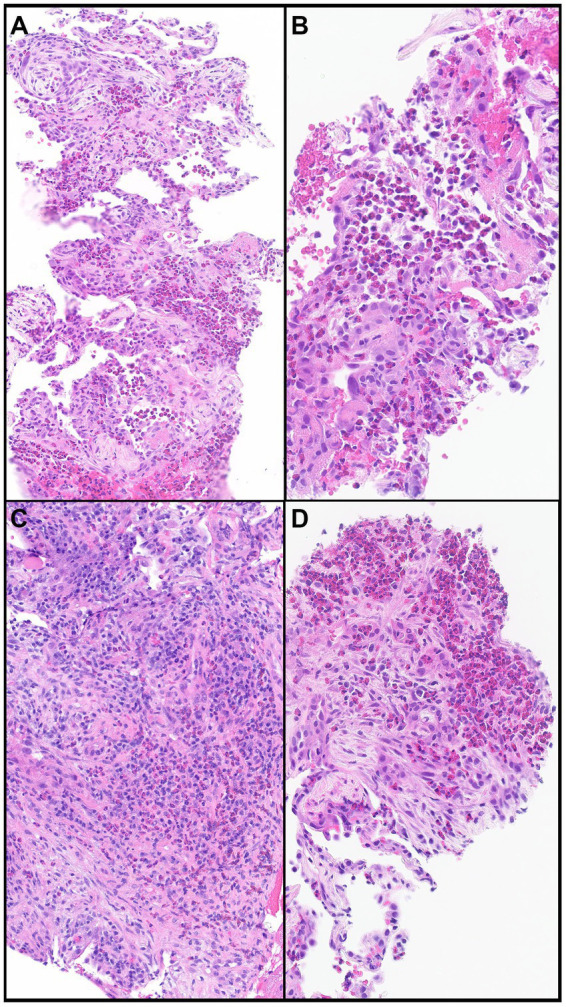
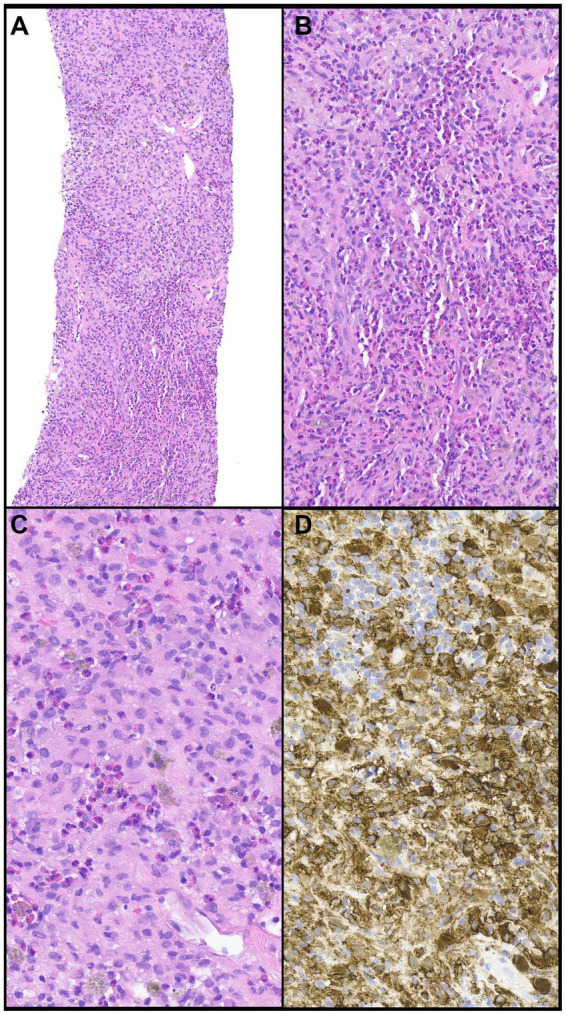
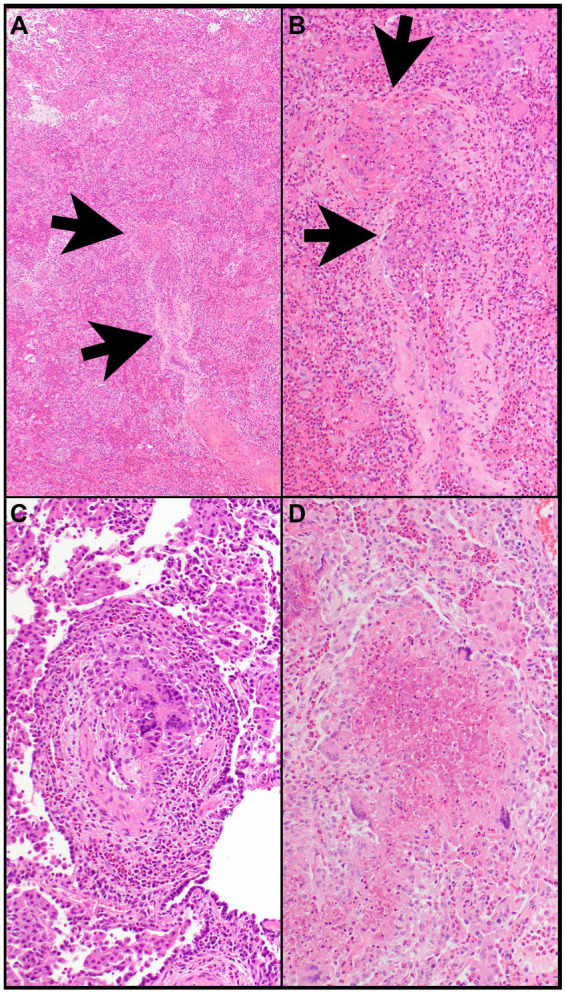
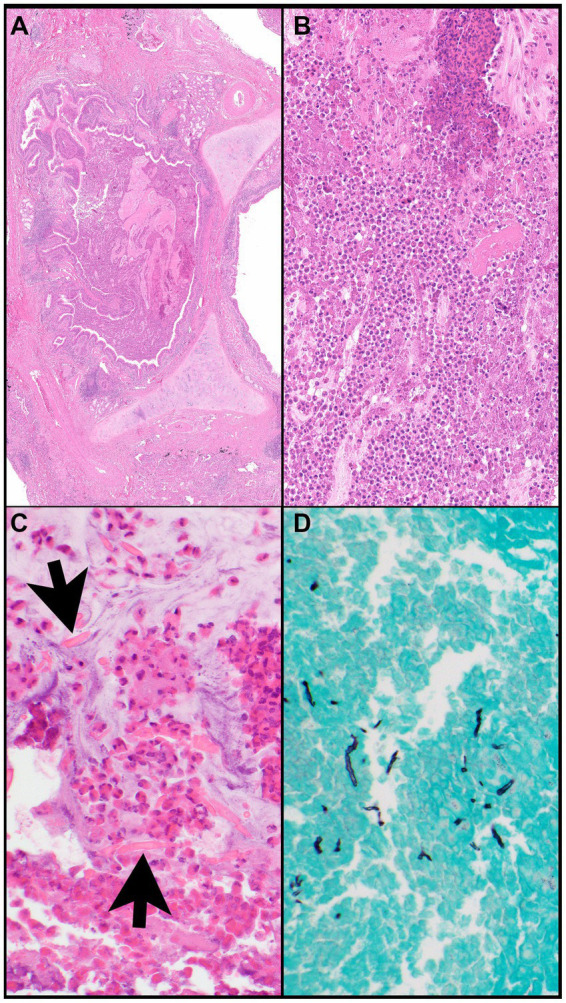
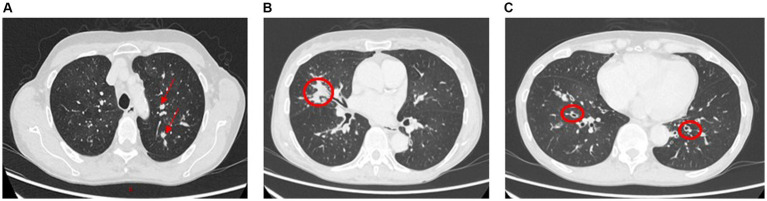
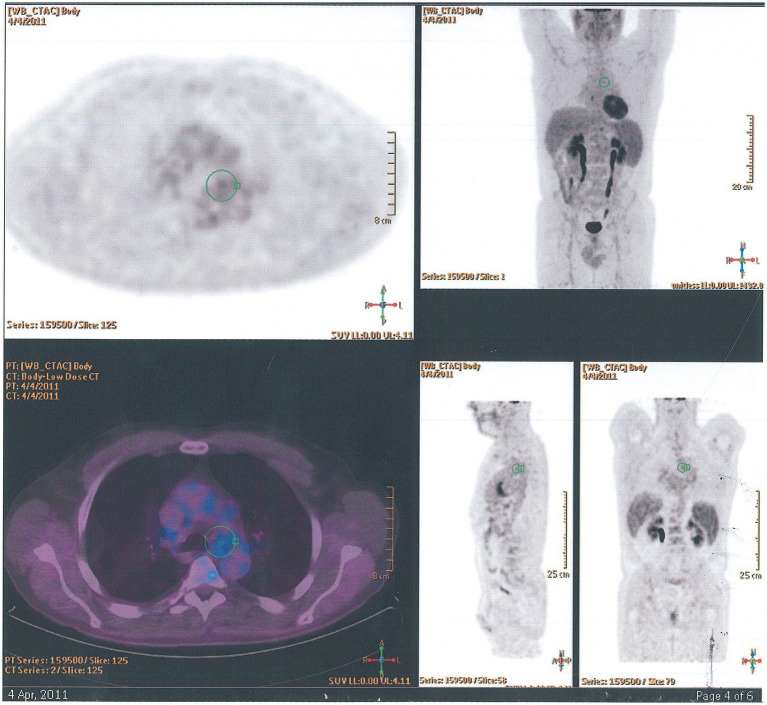
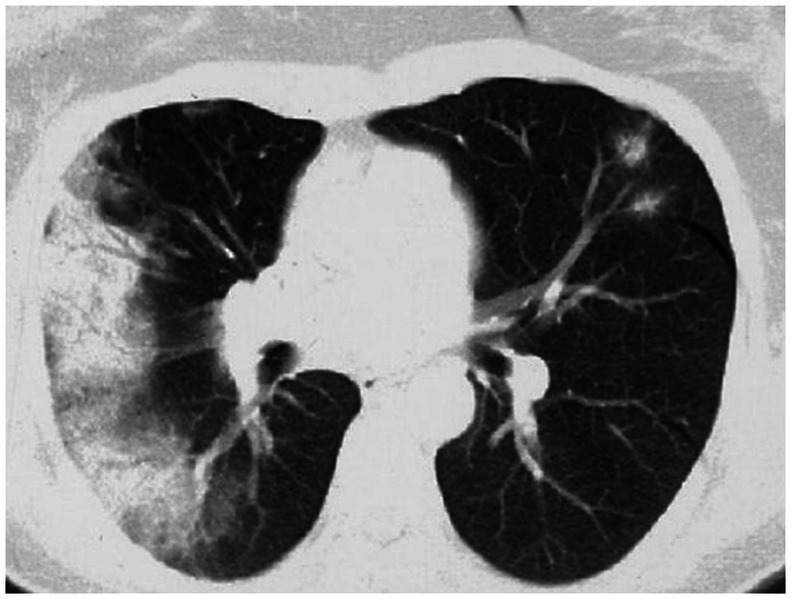
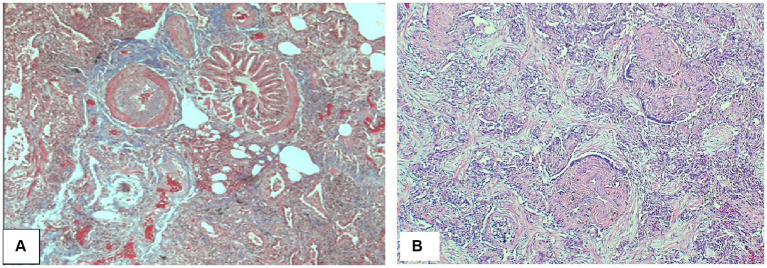
Acute and chronic eosinophilic pneumonia (AEP and CEP) include a group of rare interstitial lung diseases characterized by peripheral blood eosinophilia, increased eosinophils in bronchoalveolar lavage fluid, or eosinophilic infiltration of lung parenchyma. AEP is characterized by rapid onset, fast response to steroid treatment, and no relapse. CEP is characterized by marked tissue and peripheral blood eosinophilia, rapid response to steroid therapy, and tendency to disease recurrence. In addition, we briefly describe other eosinophilic lung diseases that must be considered in differential diagnosis of AEP and CEP. Eosinophilic pneumonias may be idiopathic or due to known causes such as medications or environmental exposure. At variance with previous reviews on this topic, a particular look in this overview was directed at pathological findings and radiological patterns.
Keywords: acute eosinophilic pneumonia; chronic eosinophilic pneumonia; eosinophilic pneumonias; high resolution computed tomography; lung pathology.
Copyright © 2024 Carbone, Puppo, Mattar, Roden and Hirani.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources