

This is a preprint.
A mitochondrial surveillance mechanism activated by SRSF2 mutations in hematologic malignancies
- PMID: 38712254
- PMCID: PMC11071312
- DOI: 10.1101/2023.06.25.546449
A mitochondrial surveillance mechanism activated by SRSF2 mutations in hematologic malignancies
Update in
-
A mitochondrial surveillance mechanism activated by SRSF2 mutations in hematologic malignancies.J Clin Invest. 2024 May 7;134(12):e175619. doi: 10.1172/JCI175619. J Clin Invest. 2024. PMID: 38713535 Free PMC article.
Abstract
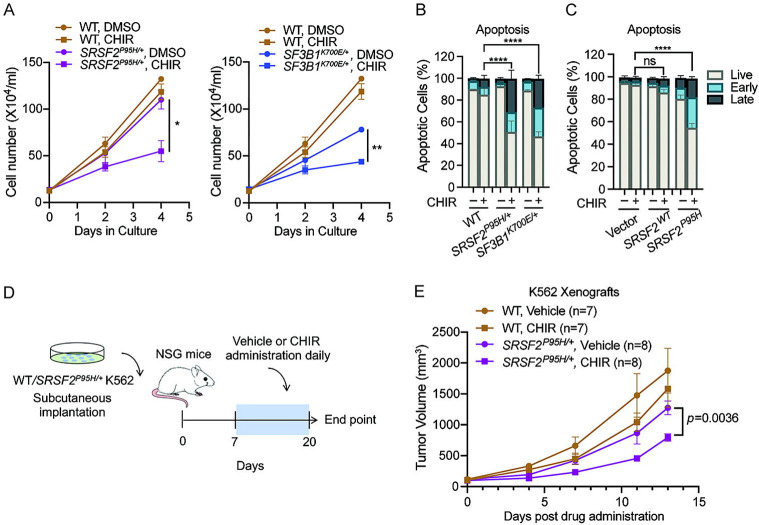
Splicing factor mutations are common in myelodysplastic syndrome (MDS) and acute myeloid leukemia (AML), but how they alter cellular functions is unclear. We show that the pathogenic SRSF2P95H/+ mutation disrupts the splicing of mitochondrial mRNAs, impairs mitochondrial complex I function, and robustly increases mitophagy. We also identified a mitochondrial surveillance mechanism by which mitochondrial dysfunction modifies splicing of the mitophagy activator PINK1 to remove a poison intron, increasing the stability and abundance of PINK1 mRNA and protein. SRSF2P95H-induced mitochondrial dysfunction increased PINK1 expression through this mechanism, which is essential for survival of SRSF2P95H/+ cells. Inhibition of splicing with a glycogen synthase kinase 3 inhibitor promoted retention of the poison intron, impairing mitophagy and activating apoptosis in SRSF2P95H/+ cells. These data reveal a homeostatic mechanism for sensing mitochondrial stress through PINK1 splicing and identify increased mitophagy as a disease marker and a therapeutic vulnerability in SRSF2P95H mutant MDS and AML.
Conflict of interest statement
Conflict of Interest Statement: PSK is collaborating with Blueprint Medicines under a sponsored research agreement unrelated to the current manuscript. OA-W has served as a consultant for H3B Biomedicine, Foundation Medicine Inc, Merck, Prelude Therapeutics, and Janssen, and is on the Scientific Advisory Board of Envisagenics Inc, AIChemy, Harmonic Discovery Inc, and Pfizer Boulder; OA-W has received prior research funding from H3B Biomedicine, Nurix Therapeutics, Minovia Therapeutics, and LOXO Oncology unrelated to the current manuscript. DCW is on the Scientific Advisory Boards of Pano Therapeutics and Medical Excellence Capital.
Figures







References
-
- Kim YJ, and Abdel-Wahab O. Therapeutic targeting of RNA splicing in myelodysplasia. Semin Hematol. 2017;54(3):167–73. - PubMed
-
- Yoshida K, Sanada M, Shiraishi Y, Nowak D, Nagata Y, Yamamoto R, et al. Frequent pathway mutations of splicing machinery in myelodysplasia. Nature. 2011;478(7367):64–9. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous