

Meta-analysis: loop ileostomy versus colostomy to prevent complications of anterior resection for rectal cancer
- PMID: 38714581
- PMCID: PMC11076370
- DOI: 10.1007/s00384-024-04639-2
Meta-analysis: loop ileostomy versus colostomy to prevent complications of anterior resection for rectal cancer
Abstract
Purpose: Anastomotic leakage is a serious complication of colorectal cancer surgery, prolonging hospital stays and impacting patient prognosis. Preventive colostomy is required in patients at risk of anastomotic fistulas. However, it remains unclear whether the commonly used loop colostomy(LC) or loop ileostomy(LI) can reduce the complications of colorectal surgery. This study aims to compare perioperative morbidities associated with LC and LI following anterior rectal cancer resection, including LC and LI reversal.
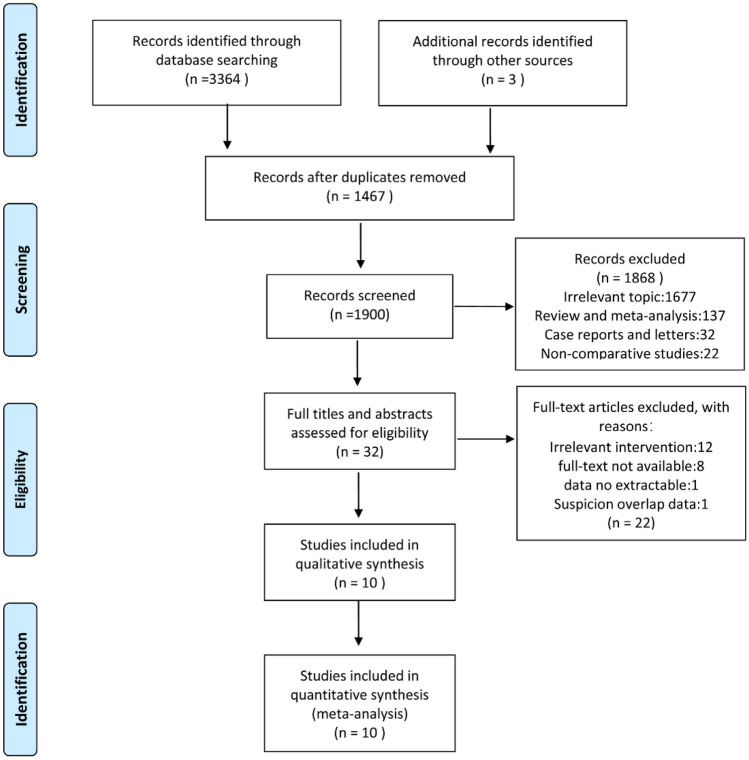
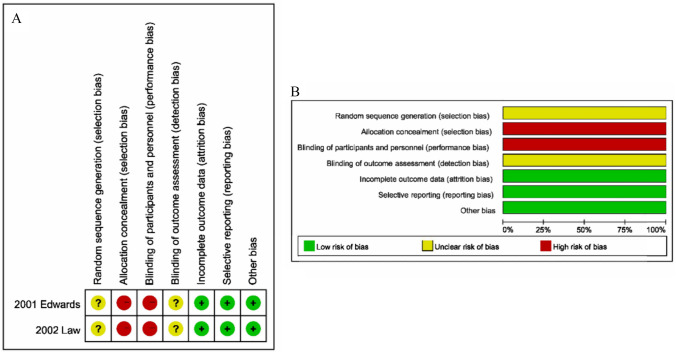
Methods: In this meta-analysis, the Embase, Web of Science, Scopus, PubMed, and Cochrane Library databases were searched for prospective cohort studies, retrospective cohort studies, and randomized controlled trials (RCTs) on perioperative morbidity during stoma development and reversal up to July 2023, The meta-analysis included 10 trials with 2036 individuals (2 RCTs and 8 cohorts).
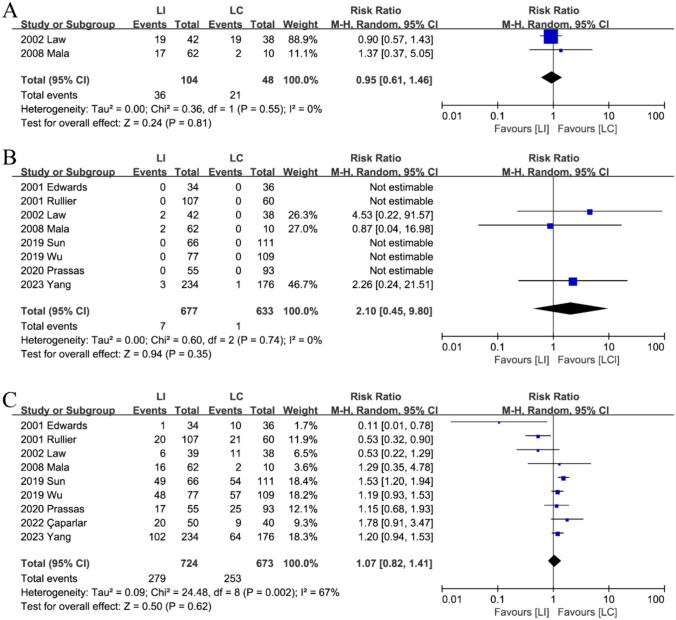
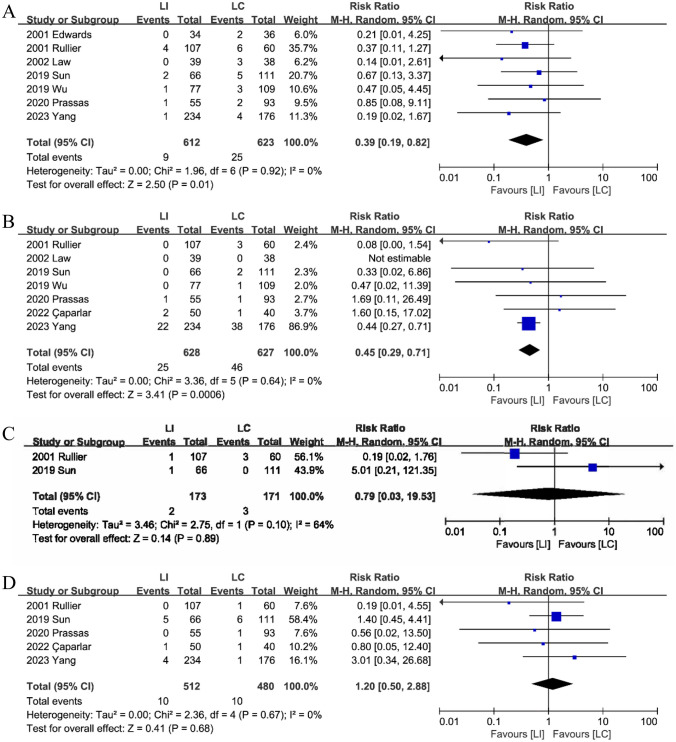
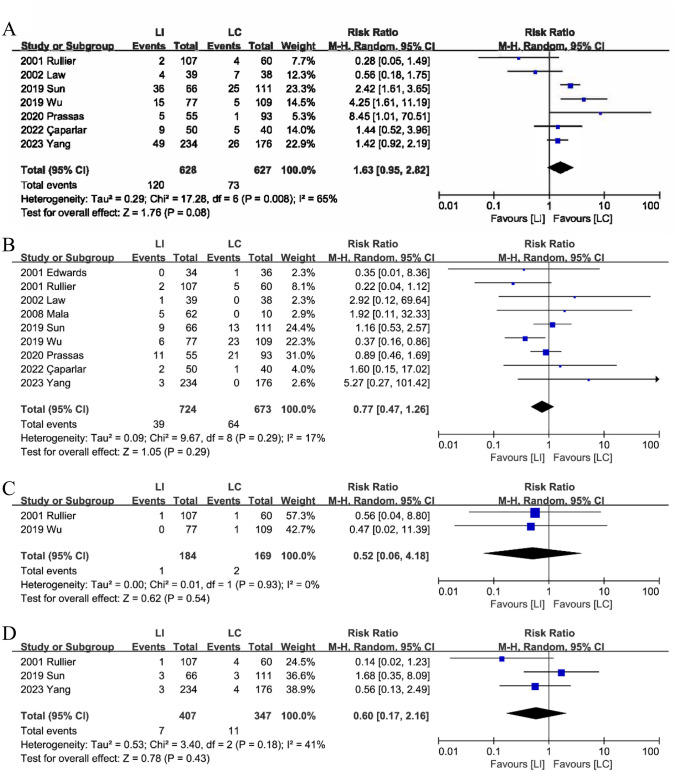
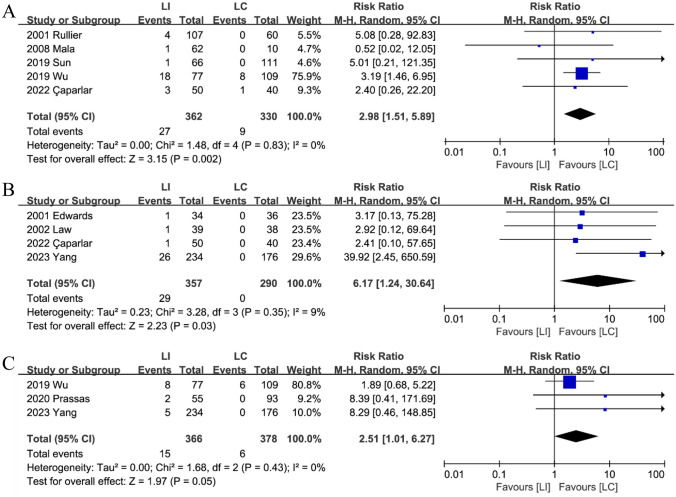
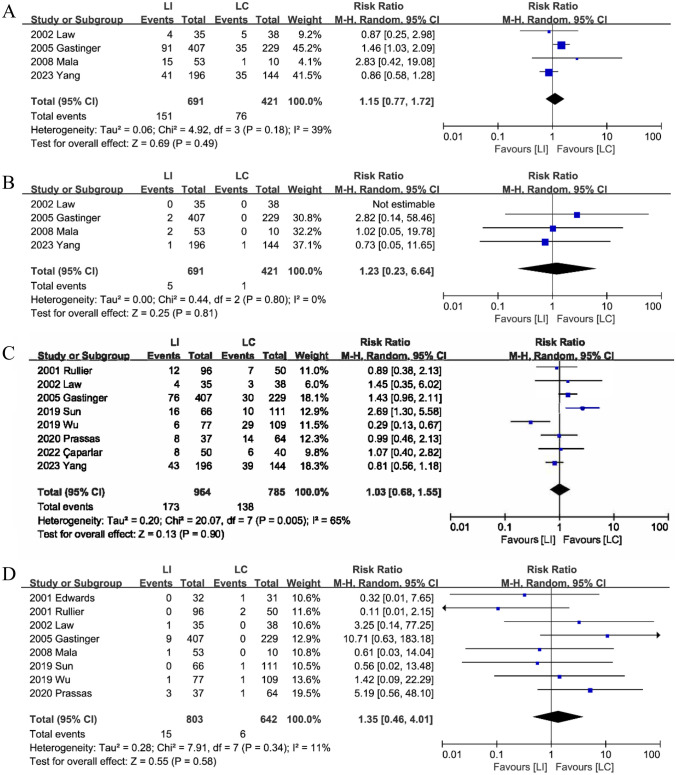
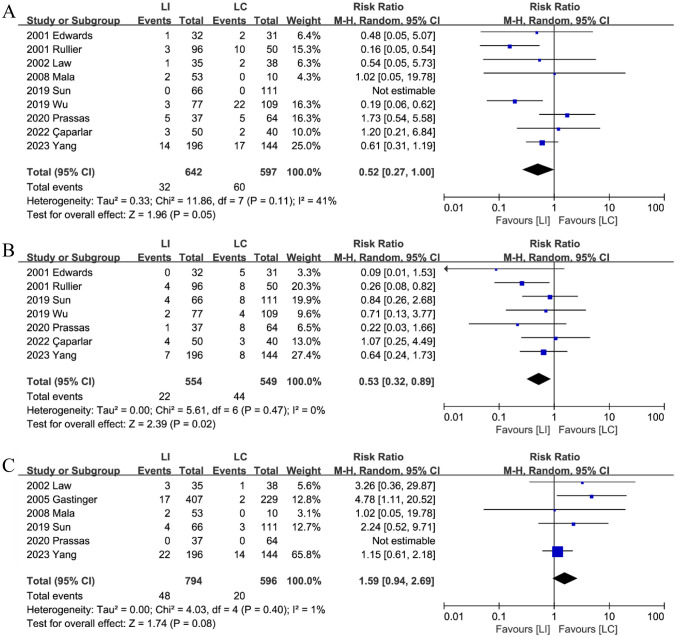
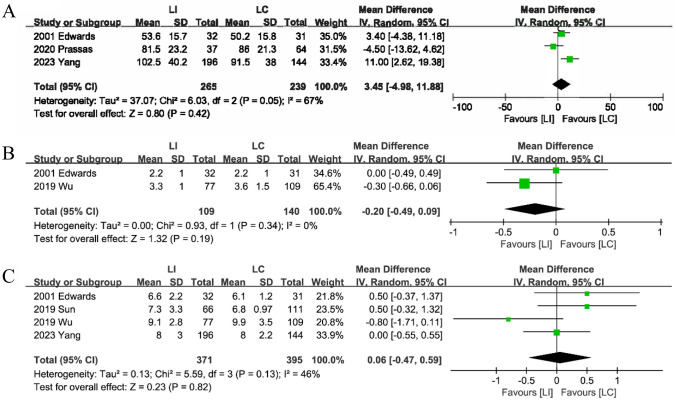
Results: No significant differences in morbidity, mortality, or stoma-related issues were found between the LI and LC groups after anterior resection surgery. However, patients in the LC group exhibited higher rates of stoma prolapse (RR: 0.39; 95%CI: 0.19-0.82; P = 0.01), retraction (RR: 0.45; 95%CI: 0.29-0.71; P < 0.01), surgical site infection (RR: 0.52; 95%CI: 0.27-1.00; P = 0.05) and incisional hernias (RR: 0.53; 95%CI: 0.32-0.89; P = 0.02) after stoma closure compared to those in the LI group. Conversely, the LI group showed higher rates of dehydration or electrolyte imbalances(RR: 2.98; 95%CI: 1.51-5.89; P < 0.01), high-output(RR: 6.17; 95%CI: 1.24-30.64; P = 0.03), and renal insufficiency post-surgery(RR: 2.51; 95%CI: 1.01-6.27; P = 0.05).
Conclusion: Our study strongly recommends a preventive LI for anterior resection due to rectal cancer. However, ileostomy is more likely to result in dehydration, renal insufficiency, and intestinal obstruction. More multicenter RCTs are needed to corroborate this.
Keywords: Anastomotic leakage; Colorectal cancer; Loop colostomy; Loop ileostomy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Heald RJ (1979) A new approach to rectal cancer. Br J Hosp Med 22(3):277–281 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
