

High SARS-CoV-2 incidence and asymptomatic fraction during Delta and Omicron BA.1 waves in The Gambia
- PMID: 38714680
- PMCID: PMC11076623
- DOI: 10.1038/s41467-024-48098-3
High SARS-CoV-2 incidence and asymptomatic fraction during Delta and Omicron BA.1 waves in The Gambia
Abstract
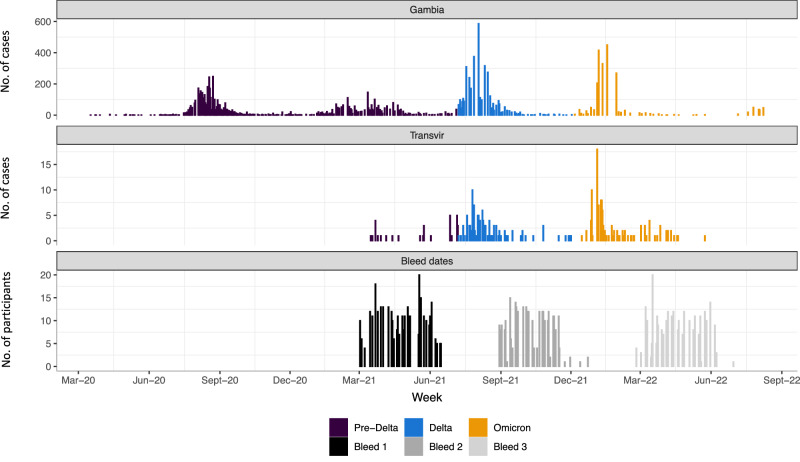
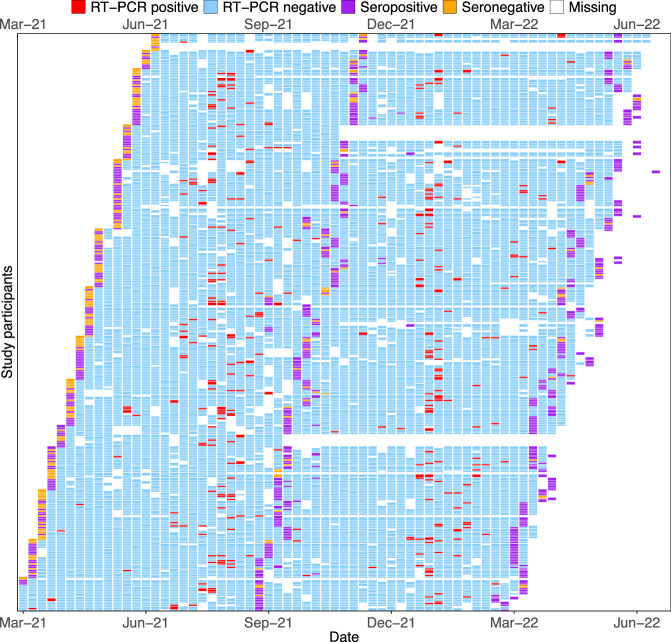
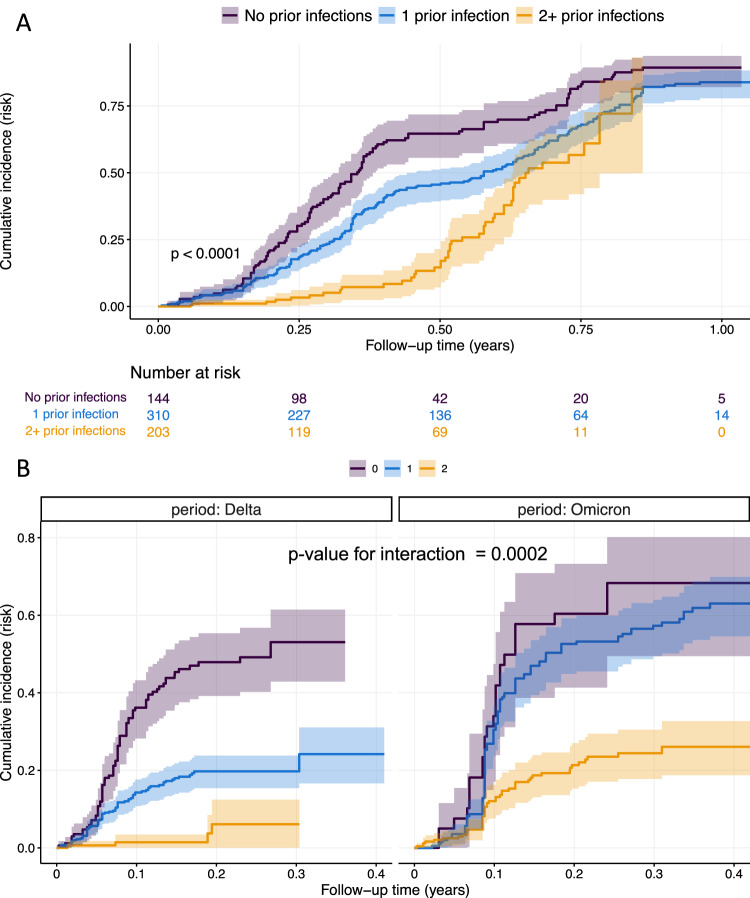
Little is known about SARS-CoV-2 infection risk in African countries with high levels of infection-driven immunity and low vaccine coverage. We conducted a prospective cohort study of 349 participants from 52 households in The Gambia between March 2021 and June 2022, with routine weekly SARS-CoV-2 RT-PCR and 6-monthly SARS-CoV-2 serology. Attack rates of 45% and 57% were seen during Delta and Omicron BA.1 waves respectively. Eighty-four percent of RT-PCR-positive infections were asymptomatic. Children under 5-years had a lower incidence of infection than 18-49-year-olds. One prior SARS-CoV-2 infection reduced infection risk during the Delta wave only, with immunity from ≥2 prior infections required to reduce the risk of infection with early Omicron lineage viruses. In an African population with high levels of infection-driven immunity and low vaccine coverage, we find high attack rates during SARS-CoV-2 waves, with a high proportion of asymptomatic infections and young children remaining relatively protected from infection.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
