

Personalized mechanical ventilation guided by ultrasound in patients with acute respiratory distress syndrome (PEGASUS): study protocol for an international randomized clinical trial
- PMID: 38715118
- PMCID: PMC11077821
- DOI: 10.1186/s13063-024-08140-7
Personalized mechanical ventilation guided by ultrasound in patients with acute respiratory distress syndrome (PEGASUS): study protocol for an international randomized clinical trial
Abstract
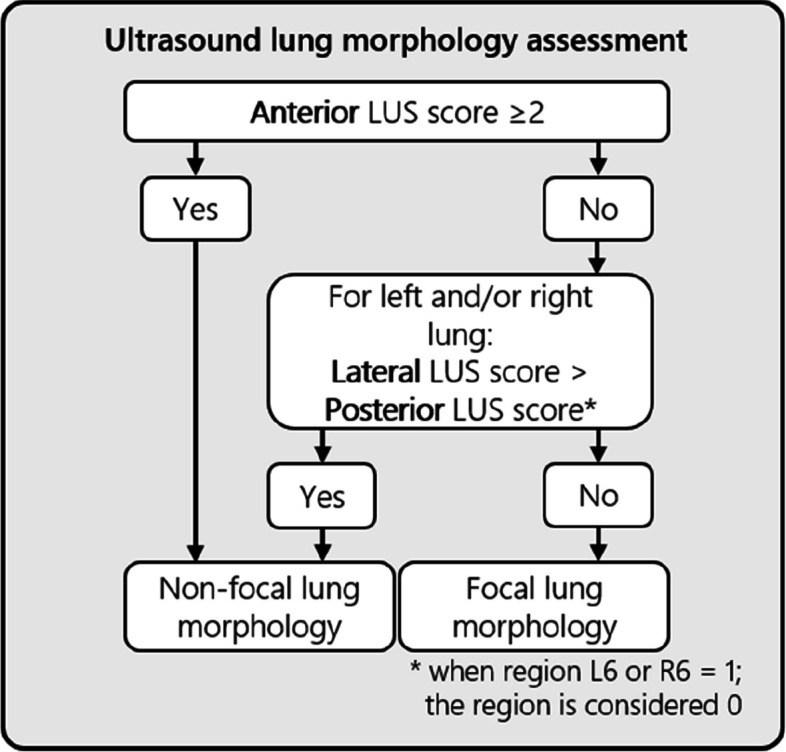
Background: Acute respiratory distress syndrome (ARDS) is a frequent cause of hypoxemic respiratory failure with a mortality rate of approximately 30%. Identifying ARDS subphenotypes based on "focal" or "non-focal" lung morphology has the potential to better target mechanical ventilation strategies of individual patients. However, classifying morphology through chest radiography or computed tomography is either inaccurate or impractical. Lung ultrasound (LUS) is a non-invasive bedside tool that can accurately distinguish "focal" from "non-focal" lung morphology. We hypothesize that LUS-guided personalized mechanical ventilation in ARDS patients leads to a reduction in 90-day mortality compared to conventional mechanical ventilation.
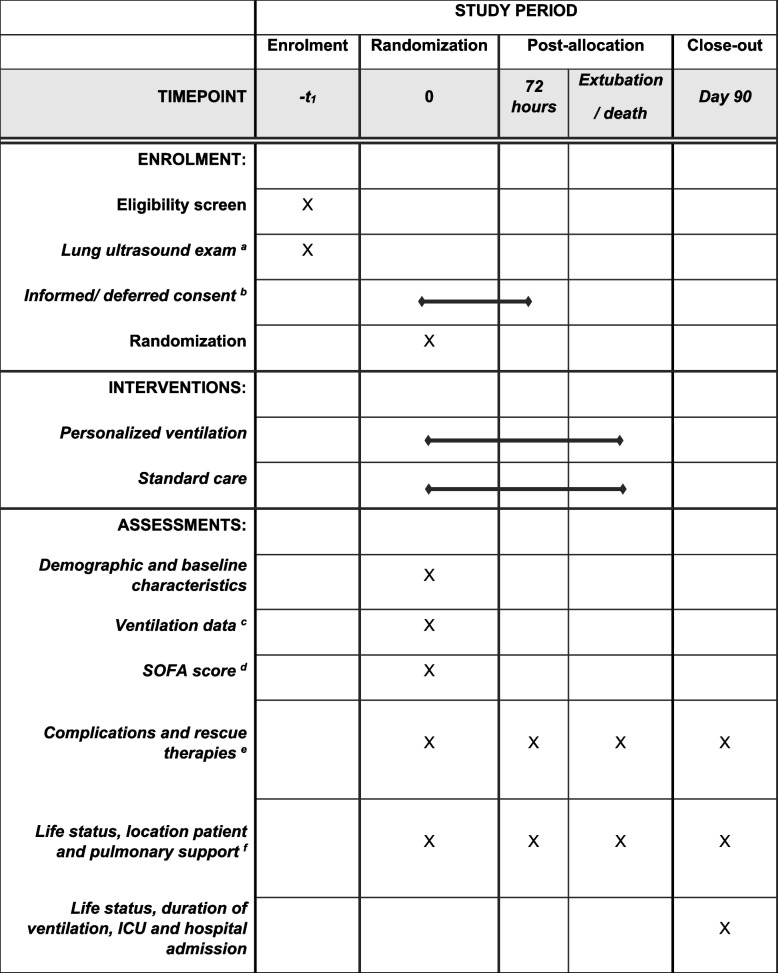
Methods: The Personalized Mechanical Ventilation Guided by UltraSound in Patients with Acute Respiratory Distress Syndrome (PEGASUS) study is an investigator-initiated, international, randomized clinical trial (RCT) that plans to enroll 538 invasively ventilated adult intensive care unit (ICU) patients with moderate to severe ARDS. Eligible patients will receive a LUS exam to classify lung morphology as "focal" or "non-focal". Thereafter, patients will be randomized within 12 h after ARDS diagnosis to receive standard care or personalized ventilation where the ventilation strategy is adjusted to the morphology subphenotype, i.e., higher positive end-expiratory pressure (PEEP) and recruitment maneuvers for "non-focal" ARDS and lower PEEP and prone positioning for "focal" ARDS. The primary endpoint is all-cause mortality at day 90. Secondary outcomes are mortality at day 28, ventilator-free days at day 28, ICU length of stay, ICU mortality, hospital length of stay, hospital mortality, and number of complications (ventilator-associated pneumonia, pneumothorax, and need for rescue therapy). After a pilot phase of 80 patients, the correct interpretation of LUS images and correct application of the intervention within the safe limits of mechanical ventilation will be evaluated.
Discussion: PEGASUS is the first RCT that compares LUS-guided personalized mechanical ventilation with conventional ventilation in invasively ventilated patients with moderate and severe ARDS. If this study demonstrates that personalized ventilation guided by LUS can improve the outcomes of ARDS patients, it has the potential to shift the existing one-size-fits-all ventilation strategy towards a more individualized approach.
Trial registration: The PEGASUS trial was registered before the inclusion of the first patient, https://clinicaltrials.gov/ (ID: NCT05492344).
Keywords: Acute respiratory distress syndrome; Lung ultrasound; Mechanical ventilation; Personalized medicine.
© 2024. The Author(s).
Conflict of interest statement
All conflicts of interests are outside the submitted work and none are considered as a competing interest. PP: Honoraria for lectures and advisory boards from Abionic, Merck Sharp & Dohme, Sanofi, Gilead, Mundipharma and Pfizer. TI: The department of anesthesiology and intensive care has a collaboration with Radiometer, Søborg, Denmark, whereby the department is reimbursed for completion of studies. TI has not received any personal payments or benefits from Radiometer. OR received a research grant from Hamilton Medical AG and Fisher&Paykel Healthcare Ltd, speaker fees from Hamilton Medical AG, Fisher&Paykel Healthcare Ltd, Aerogen Ltd and Ambu, and non-financial research support from Timpel.
Figures

References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
