

Predictive factors for complexity in abdominal wall hernias: a literature scope review
- PMID: 38716916
- PMCID: PMC11185061
- DOI: 10.1590/0100-6991e-20243670-en
Predictive factors for complexity in abdominal wall hernias: a literature scope review
Abstract
Introduction: Abdominal wall hernias encompass both ventral and incisional hernias, often poorly classified regarding complexity in general. This study aims to conduct a review on the primary topics related to defining the complexity of ventral hernias.
Methods: this is a scope review conducted following the guidelines recommended by the PRISMA-ScR directive. Searches were carried out in electronic databases including PubMed, LILACS, and EMBASE, using the descriptors: Abdominal Hernia, Hernia, Ventral Hernia, Incisional Hernia, Complex, Classification, Classify, Grade, Scale, and Definition. Combinations of these terms were employed when appropriate. Inclusion criteria encompassed articles with definitions and classifications of complex hernias, as well as those utilizing these classifications to guide treatments and patient allocation. Synonyms and related topics were also considered. Articles outside the scope or lacking the themes in their title or abstract were excluded. The database search was conducted up to July 29, 2023.
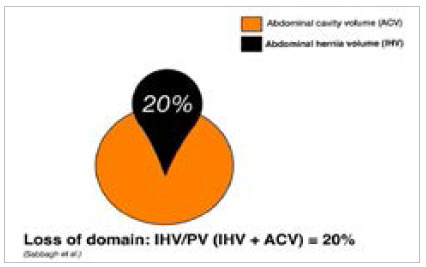
Results: several hernia classifications were identified as useful in predicting complexity. For this study, we considered six main criteria: size and location, loss of domain, use of abdominal wall relaxation techniques, characteristics of imaging exams, status of the subcutaneous cellular tissue, and likelihood of recurrence.
Conclusion: complex abdominal wall hernias can be defined by characteristics analyzed collectively, relating to the patients previous clinical status, size and location of the hernia defect, status of subcutaneous cellular tissue, myofascial release techniques, and other complicating factors.
Introdução:: As hérnias da parede abdominal, englobam em seu conceito as hérnias ventrais e incisionais. Essas hérnias são mal classificadas quanto à complexidade de forma geral. Esse estudo tem por objetivo realizar uma revisão sobre os principais tópicos relacionados à definição de complexidade das hérnias ventrais.
Métodos:: trata-se de revisão de escopo realizada com as orientações preconizadas pela diretriz PRISMA-ScR. Foram realizadas buscas nas bases de dados eletrônicas do PubMed, LILACS e EMBASE, empregando os descritores: “Abdominal Hernia”; Hernia; “Ventral Hernia”; “Incisional Hernia”; Complex; Classification, Classify, Grade, Scale e definition. Combinações entre os termos foram utilizadas quando oportunas. Os critérios de inclusão abrangiam artigos com definições e classificações de hérnias complexas, além daqueles que usavam essas classificações para orientar tratamentos e alocação de pacientes. Sinônimos e tópicos relacionados também foram considerados. Artigos fora do escopo ou sem os temas no título ou resumo foram excluídos. A busca nas bases de dados foi realizada até o dia 29/07/2023.
Resultados:: diversas classificações de hérnias foram identificadas como sendo úteis para prever complexidade. Consideramos para esse estudo seis critérios principais: tamanho e localização, perda de domicílio, uso de técnicas de relaxamento da parede abdominal, características dos exames de imagem, status do tecido celular subcutâneo e chance de recorrência.
Conclusão:: as hérnias complexas da parede abdominal podem ser definidas por características analisadas conjuntamente e que estão relacionadas ao estado clínico prévio do paciente, tamanho e localização do defeito herniário, status do tecido celular subcutâneo, técnicas de liberação miofascial e outros fatores complicadores..
Conflict of interest statement
Conflict of interest: no.
Figures





References
-
- Chevrel JP, Rath AM. Classification of incisional hernias of the abdominal wall. Hernia. 2000;4:7–11.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
