

Human shoulder anatomy: new ultrasound, anatomical, and microscopic perspectives
- PMID: 38717695
- PMCID: PMC11142962
- DOI: 10.1007/s12565-024-00775-5
Human shoulder anatomy: new ultrasound, anatomical, and microscopic perspectives
Abstract
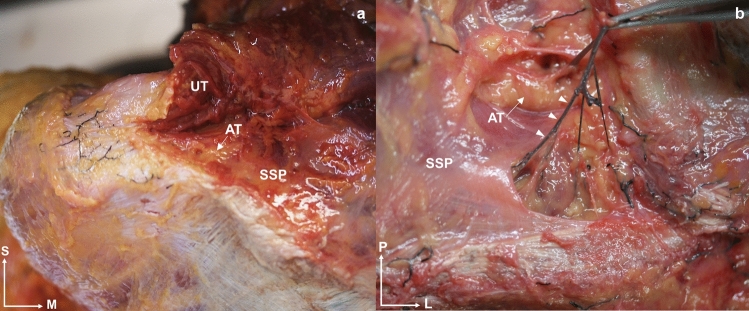
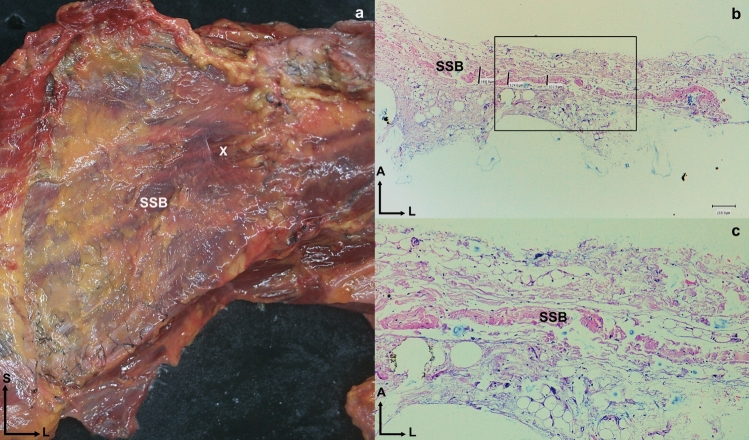
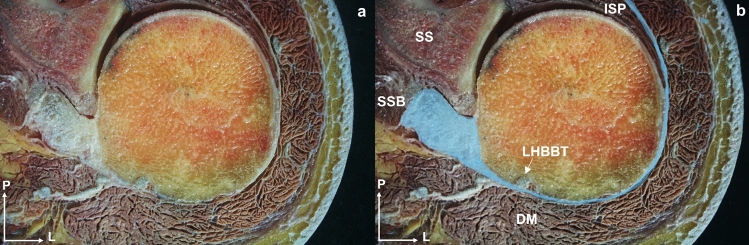
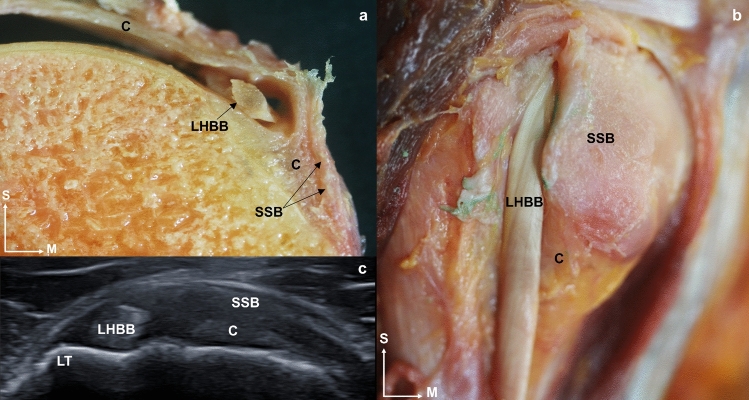
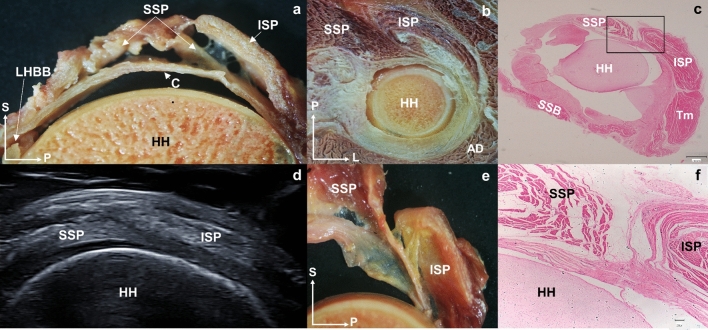
This study aimed to describe the shoulder anatomy, together with the anatomical relationships in adults and early stages of development. The shoulder muscles were studied from ultrasound, anatomical, and microscopic perspectives in a sample of 34 human shoulders. Thickness measurements were taken of the tendons and fasciae of the subscapularis, long head tendon of the biceps brachii, supraspinatus, infraspinatus, and teres minor. Ultrasound and dissection techniques are strongly correlated. However, the measurements obtained from the dissection technique were superior to those obtained from the ultrasound in all cases, except for the thickness of the long head tendon of the biceps brachii, the teres minor tendon, and the fascia thickness of the infraspinatus. In addition, the study of shoulder anatomy revealed no differences between females and males. Relevant findings from dissection included a clear overlap between the infraspinatus and supraspinatus, which shared tendon fibers, and a similar connection between the transverse ligament of the long head tendon of the biceps brachii and the subscapularis, which created a more interconnected shoulder function. The study of the anatomical measurements shows an underestimation of the shoulder measurements in the ultrasound compared with the dissection technique, but a high correlation between the measurements made by the two techniques. We present reference values for the tendon and fascia thicknesses of the rotator cuff, with no differences observed by gender. The relationships between shoulder structures described in the anatomical study imply as well that, in the event of an injury, adjacent tissues may be affected. This extended information may facilitate future optimal clinical explorations.
Keywords: Anatomy; Muscular fascia; Rotator cuff; Tendon; Ultrasound imaging.
© 2024. The Author(s).
Conflict of interest statement
All authors certify that they have no affiliations with or involvement in any organization or entity with a financial or non-financial interest in the subject matter or materials discussed in this manuscript.
Figures








References
-
- Bağcier B, Geler Külcü GK, Yorulmaz Y, Altunok ÇA. Intra- and inter-rater reliability of ultrasound measurements of supraspinatus tendon thickness, acromiohumeral distance, and occupation ratio in patients with shoulder impingement syndrome. Arch Rheumatol. 2020;35:385. doi: 10.46497/ArchRheumatol.2020.7515. - DOI - PMC - PubMed
