

Development and Implementation of a Digital Quality Measure of Emergency Cancer Diagnosis
- PMID: 38718321
- PMCID: PMC11268555
- DOI: 10.1200/JCO.23.01523
Development and Implementation of a Digital Quality Measure of Emergency Cancer Diagnosis
Abstract
Purpose: Missed and delayed cancer diagnoses are common, harmful, and often preventable. Automated measures of quality of cancer diagnosis are lacking but could identify gaps and guide interventions. We developed and implemented a digital quality measure (dQM) of cancer emergency presentation (EP) using electronic health record databases of two health systems and characterized the measure's association with missed opportunities for diagnosis (MODs) and mortality.
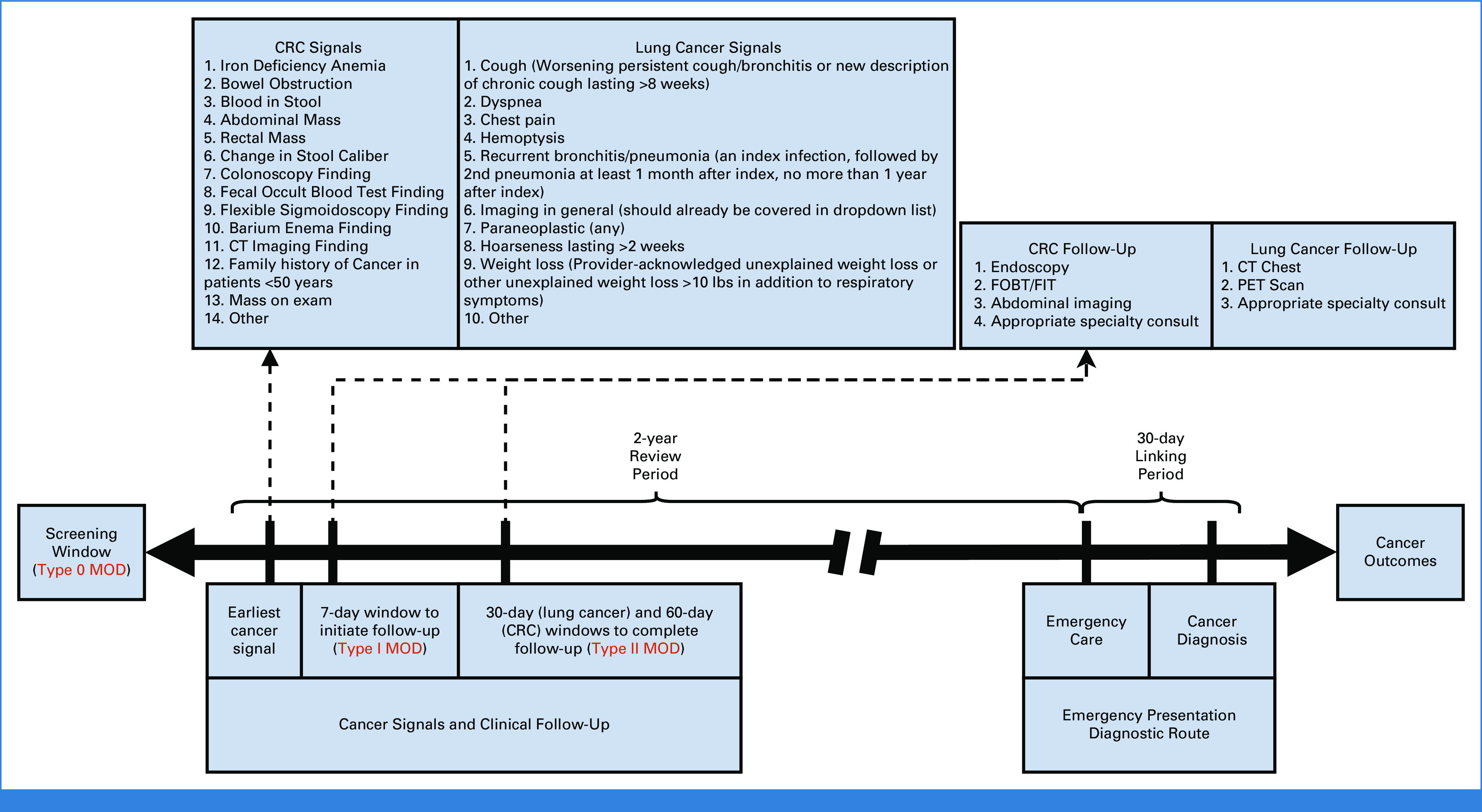
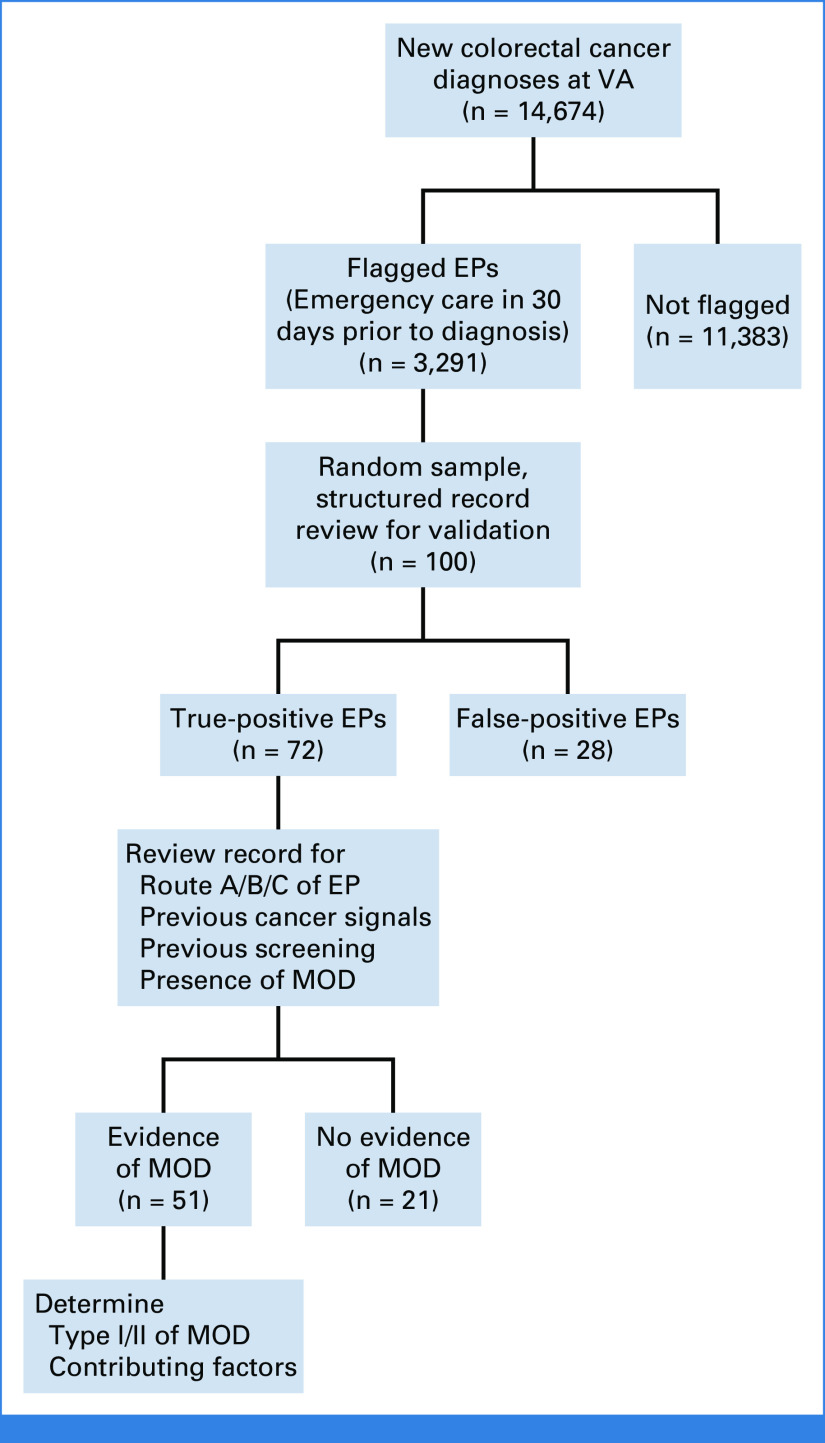
Methods: On the basis of literature and expert input, we defined EP as a new cancer diagnosis within 30 days after emergency department or inpatient visit. We identified EPs for lung cancer and colorectal cancer (CRC) in the Department of Veterans Affairs (VA) and Geisinger from 2016 to 2020. We validated measure accuracy and identified preceding MODs through standardized chart review of 100 records per cancer per health system. Using VA's longitudinal encounter and mortality data, we applied logistic regression to assess EP's association with 1-year mortality, adjusting for cancer stage and demographics.
Results: Among 38,565 and 2,914 patients with lung cancer and 14,674 and 1,649 patients with CRCs at VA and Geisinger, respectively, our dQM identified EPs in 20.9% and 9.4% of lung cancers, and 22.4% and 7.5% of CRCs. Chart reviews revealed high positive predictive values for EPs across sites and cancer types (72%-90%), and a substantial percent represented MODs (48.8%-84.9%). EP was associated with significantly higher odds of 1-year mortality for lung cancer and CRC (adjusted odds ratio, 1.78 and 1.83, respectively, 95% CI, 1.63 to 1.86 and 1.61 to 2.07).
Conclusion: A dQM for cancer EP was strongly associated with both mortality and MODs. The findings suggest a promising automated approach to measuring quality of cancer diagnosis in US health systems.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures
References
-
- Newman-Toker DE, Schaffer AC, Yu-Moe CW, et al. Serious misdiagnosis-related harms in malpractice claims: The “Big Three”—Vascular events, infections, and cancers. Diagnosis. 2019;6:227–240. - PubMed
-
- Gandhi TK, Kachalia A, Thomas EJ, et al. Missed and delayed diagnoses in the ambulatory setting: A study of closed malpractice claims. Ann Intern Med. 2006;145:488–496. - PubMed
-
- National Academies of Sciences, Engineering, and Medicine: Improving Diagnosis in Health Care. Washington, DC: The National Academies Press; 2015.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
