

Recombinant ADAMTS13 for Immune Thrombotic Thrombocytopenic Purpura
- PMID: 38718359
- PMCID: PMC11128310
- DOI: 10.1056/NEJMoa2402567
Recombinant ADAMTS13 for Immune Thrombotic Thrombocytopenic Purpura
Abstract
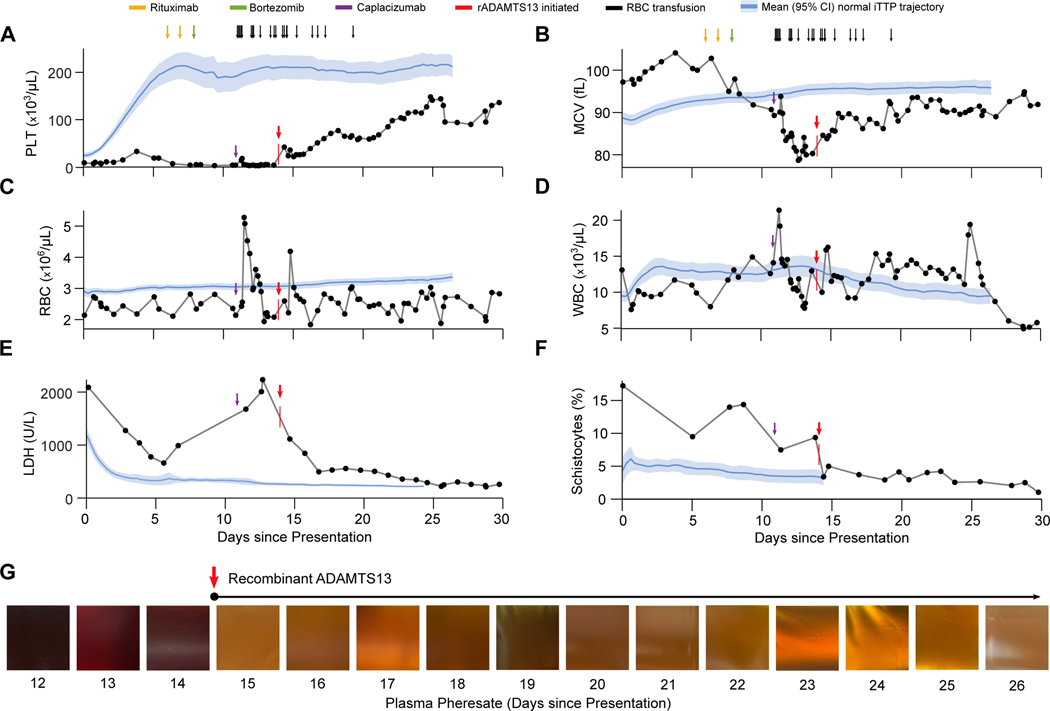
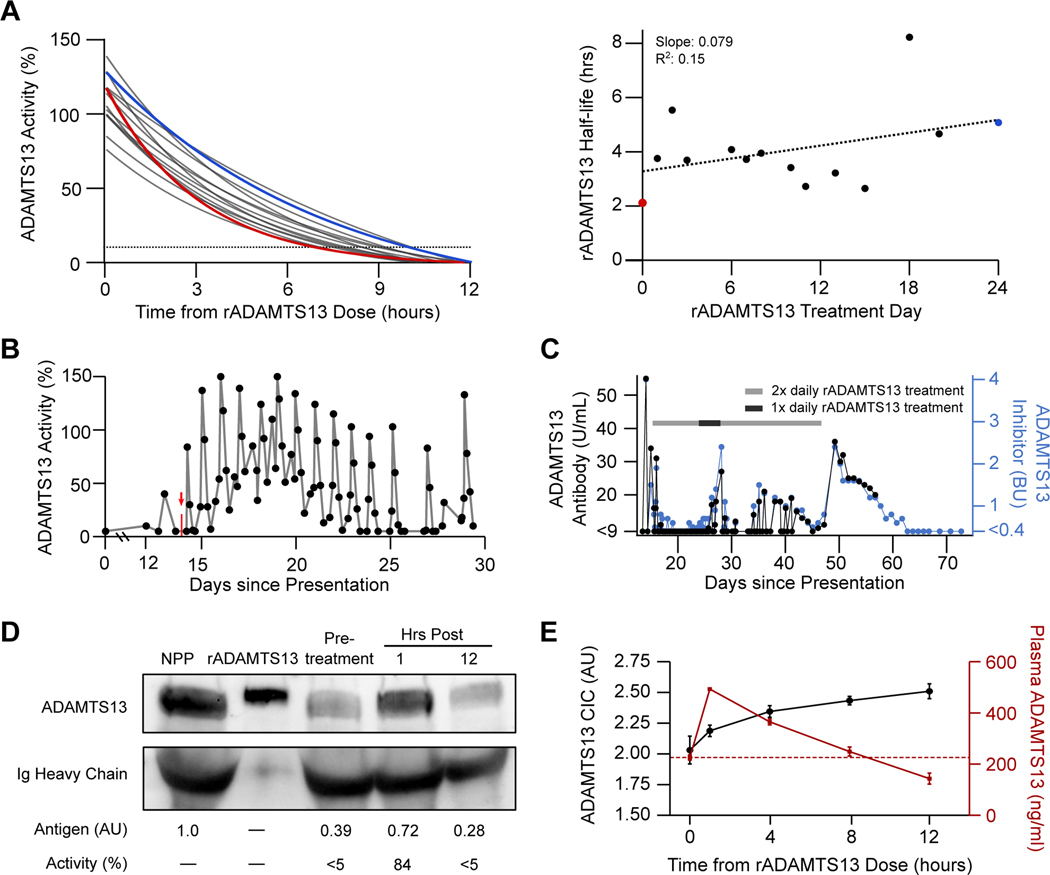
In patients with immune thrombotic thrombocytopenic purpura (iTTP), autoantibodies against the metalloprotease ADAMTS13 lead to catastrophic microvascular thrombosis. However, the potential benefits of recombinant human ADAMTS13 (rADAMTS13) in patients with iTTP remain unknown. Here, we report the clinical use of rADAMTS13, which resulted in the rapid suppression of disease activity and complete recovery in a critically ill patient whose condition had proved to be refractory to all available treatments. We also show that rADAMTS13 causes immune complex formation, which saturates the autoantibody and may promote its clearance. Our data support the role of rADAMTS13 as a novel adjunctive therapy in patients with iTTP.
Copyright © 2024 Massachusetts Medical Society.
Figures

Comment in
-
Recombinant ADAMTS13 for Immune Thrombotic Thrombocytopenic Purpura.N Engl J Med. 2024 Jul 25;391(4):382-383. doi: 10.1056/NEJMc2406975. N Engl J Med. 2024. PMID: 39047255 No abstract available.
-
Recombinant ADAMTS13 for Immune Thrombotic Thrombocytopenic Purpura.N Engl J Med. 2024 Jul 25;391(4):383. doi: 10.1056/NEJMc2406975. N Engl J Med. 2024. PMID: 39047256 No abstract available.
-
Recombinant ADAMTS13 for Immune Thrombotic Thrombocytopenic Purpura. Reply.N Engl J Med. 2024 Jul 25;391(4):383-384. doi: 10.1056/NEJMc2406975. N Engl J Med. 2024. PMID: 39047257 No abstract available.
References
-
- Mariotte E, Azoulay E, Galicier L, et al. Epidemiology and pathophysiology of adulthood-onset thrombotic microangiopathy with severe ADAMTS13 deficiency (thrombotic thrombocytopenic purpura): a cross-sectional analysis of the French national registry for thrombotic microangiopathy. The Lancet Haematology 2016;3(5):e237–45. (In eng). DOI: 10.1016/s2352-3026(16)30018-7. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases