

TLR agonists polarize interferon responses in conjunction with dendritic cell vaccination in malignant glioma: a randomized phase II Trial
- PMID: 38719809
- PMCID: PMC11078958
- DOI: 10.1038/s41467-024-48073-y
TLR agonists polarize interferon responses in conjunction with dendritic cell vaccination in malignant glioma: a randomized phase II Trial
Erratum in
-
Author Correction: TLR agonists polarize interferon responses in conjunction with dendritic cell vaccination in malignant glioma: a randomized phase II Trial.Nat Commun. 2024 Jun 5;15(1):4800. doi: 10.1038/s41467-024-48995-7. Nat Commun. 2024. PMID: 38839763 Free PMC article. No abstract available.
Abstract
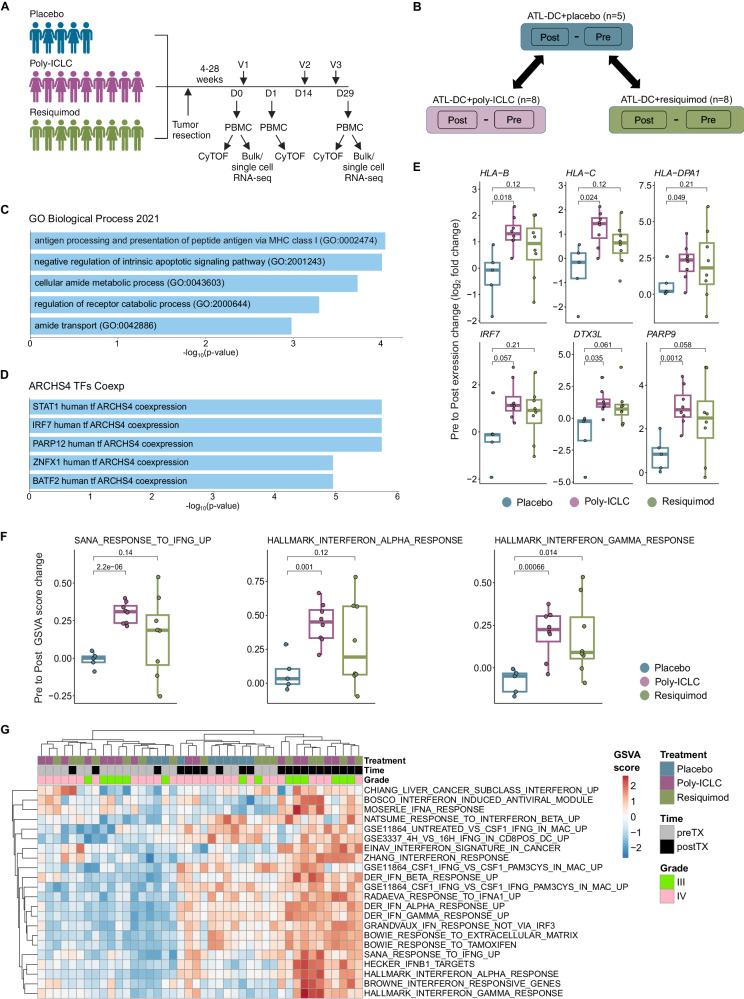
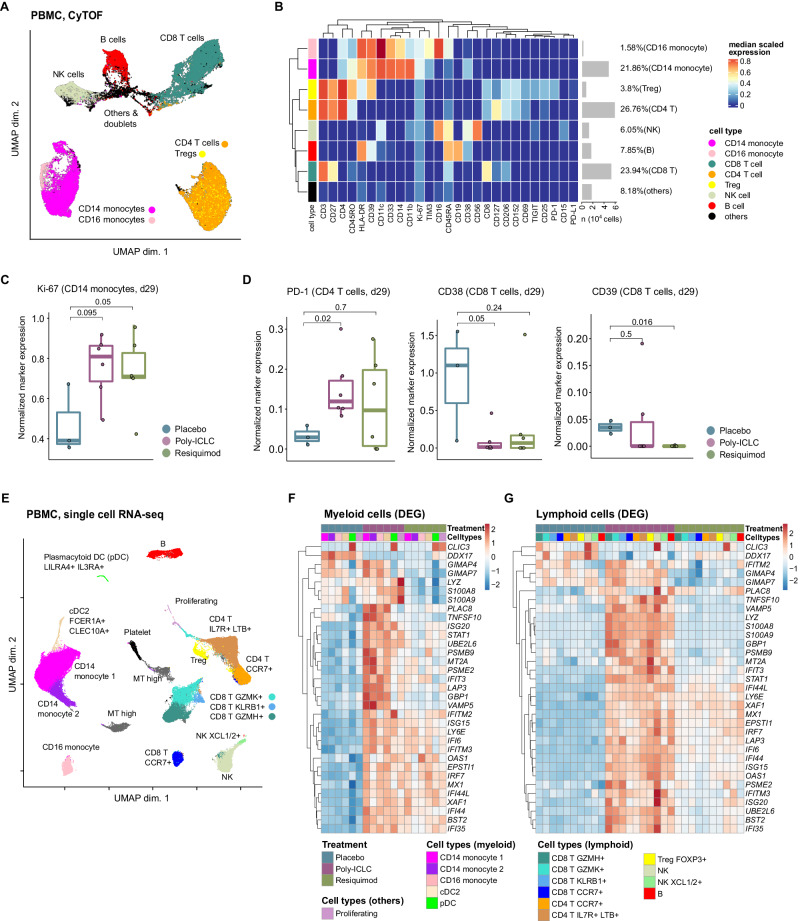
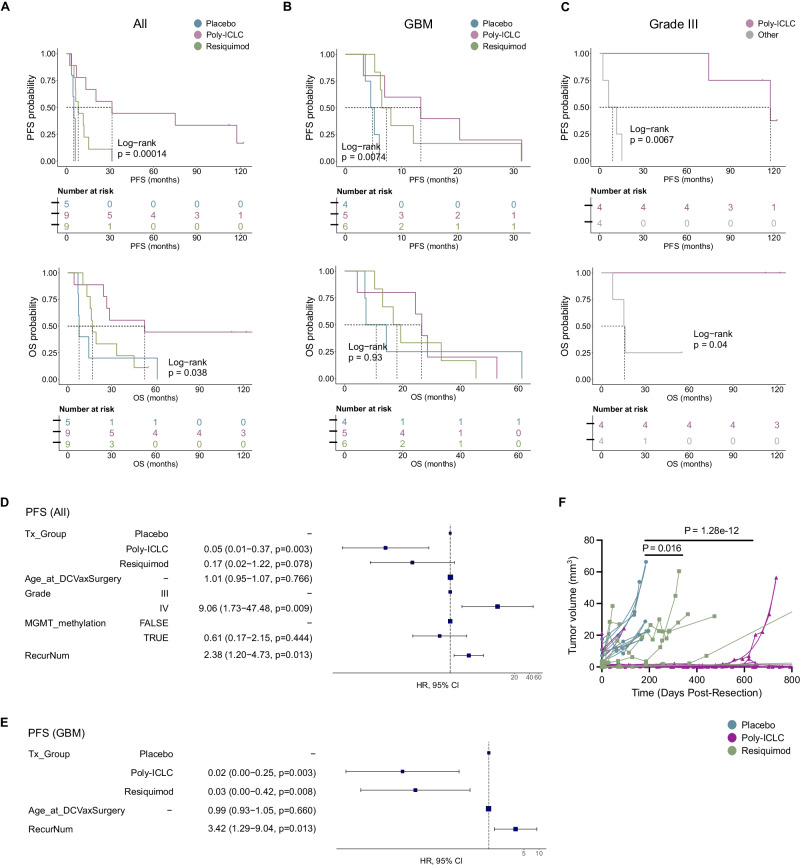
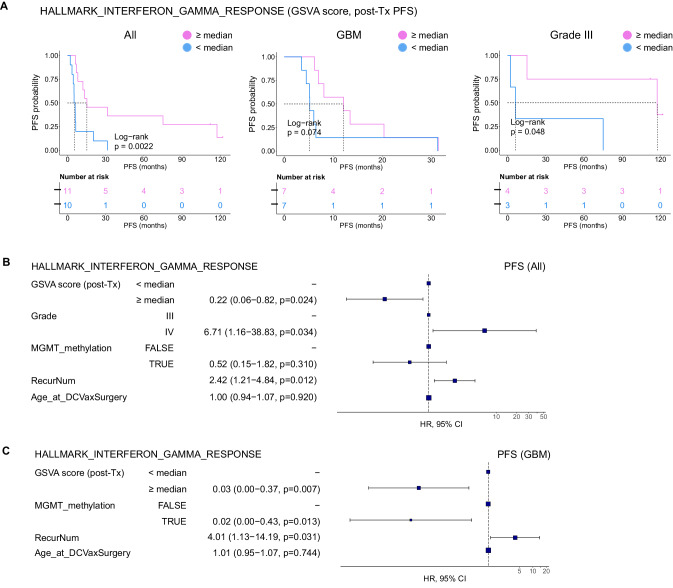
In this randomized phase II clinical trial, we evaluated the effectiveness of adding the TLR agonists, poly-ICLC or resiquimod, to autologous tumor lysate-pulsed dendritic cell (ATL-DC) vaccination in patients with newly-diagnosed or recurrent WHO Grade III-IV malignant gliomas. The primary endpoints were to assess the most effective combination of vaccine and adjuvant in order to enhance the immune potency, along with safety. The combination of ATL-DC vaccination and TLR agonist was safe and found to enhance systemic immune responses, as indicated by increased interferon gene expression and changes in immune cell activation. Specifically, PD-1 expression increases on CD4+ T-cells, while CD38 and CD39 expression are reduced on CD8+ T cells, alongside an increase in monocytes. Poly-ICLC treatment amplifies the induction of interferon-induced genes in monocytes and T lymphocytes. Patients that exhibit higher interferon response gene expression demonstrate prolonged survival and delayed disease progression. These findings suggest that combining ATL-DC with poly-ICLC can induce a polarized interferon response in circulating monocytes and CD8+ T cells, which may represent an important blood biomarker for immunotherapy in this patient population.Trial Registration: ClinicalTrials.gov Identifier: NCT01204684.
© 2024. The Author(s).
Conflict of interest statement
Andres Salazar is the Founder, CEO and Scientific Director for Oncovir, which provided the TLR agonist (Poly-ICLC) used in the trial. Linda M. Liau is a member of the Scientific Advisory Board for Northwest Bioetherapeutics, Inc, which has licensed the DC vaccine technology. All others declare no competing interests.
Figures
Update of
-
Dendritic Cell Vaccination in Conjunction with a TLR Agonist Polarizes Interferon Immune Responses in Malignant Glioma Patients.Res Sq [Preprint]. 2023 Sep 12:rs.3.rs-3287211. doi: 10.21203/rs.3.rs-3287211/v1. Res Sq. 2023. Update in: Nat Commun. 2024 May 8;15(1):3882. doi: 10.1038/s41467-024-48073-y. PMID: 37790490 Free PMC article. Updated. Preprint.
References
-
- Okada H, et al. Induction of CD8+ T-cell responses against novel glioma-associated antigen peptides and clinical activity by vaccinations with {alpha}-type 1 polarized dendritic cells and polyinosinic-polycytidylic acid stabilized by lysine and carboxymethylcellulose in patients with recurrent malignant glioma. J. Clin. Oncol. 2011;29:330–336. doi: 10.1200/JCO.2010.30.7744. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
