

CSChighE-cadherinlow immunohistochemistry panel predicts poor prognosis in oral squamous cell carcinoma
- PMID: 38719848
- PMCID: PMC11078993
- DOI: 10.1038/s41598-024-55594-5
CSChighE-cadherinlow immunohistochemistry panel predicts poor prognosis in oral squamous cell carcinoma
Abstract
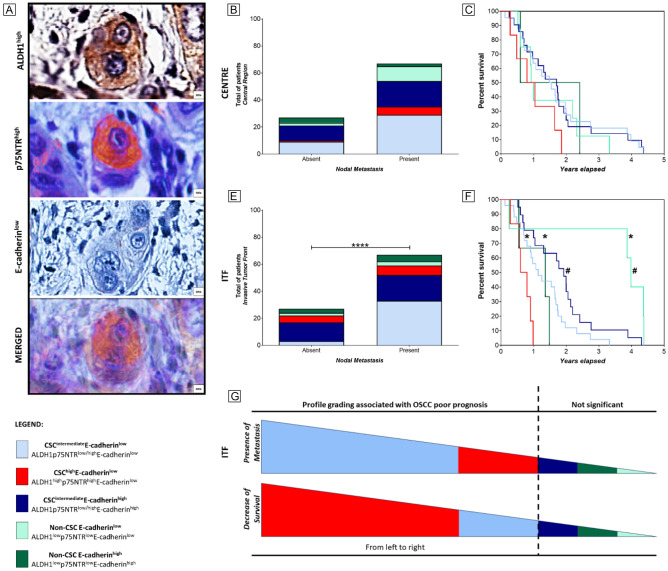
Identifying marker combinations for robust prognostic validation in primary tumour compartments remains challenging. We aimed to assess the prognostic significance of CSC markers (ALDH1, CD44, p75NTR, BMI-1) and E-cadherin biomarkers in OSCC. We analysed 94 primary OSCC and 67 metastatic lymph node samples, including central and invasive tumour fronts (ITF), along with clinicopathological data. We observed an increase in ALDH1+/CD44+/BMI-1- tumour cells in metastatic lesions compared to primary tumours. Multivariate analysis highlighted that elevated p75NTR levels (at ITF) and reduced E-cadherin expression (at the tumour centre) independently predicted metastasis, whilst ALDH1high exhibited independent predictive lower survival at the ITF, surpassing the efficacy of traditional tumour staging. Then, specifically at the ITF, profiles characterized by CSChighE-cadherinlow (ALDH1highp75NTRhighE-cadherinlow) and CSCintermediateE-cadherinlow (ALDH1 or p75NTRhighE-cadherinlow) were significantly associated with worsened overall survival and increased likelihood of metastasis in OSCC patients. In summary, our study revealed diverse tumour cell profiles in OSCC tissues, with varying CSC and E-cadherin marker patterns across primary tumours and metastatic sites. Given the pivotal role of reduced survival rates as an indicator of unfavourable prognosis, the immunohistochemistry profile identified as CSChighE-cadherinlow at the ITF of primary tumours, emerges as a preferred prognostic marker closely linked to adverse outcomes in OSCC.
Keywords: Cancer stem cells; Digital pathology; Epithelial-mesenchymal transition; Immunohistochemistry; Metastasis; Oral cancer.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Noguti J, et al. Metastasis from oral cancer: an overview. Cancer Genom. Proteom. 2012;9:329–335. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
